
 I have been a student of our bureaucracies for some 40 yrs.. They very seldom do anything in a “one and done” type approach… particularly when a large part of the population is going to be directly affected.
I have been a student of our bureaucracies for some 40 yrs.. They very seldom do anything in a “one and done” type approach… particularly when a large part of the population is going to be directly affected.
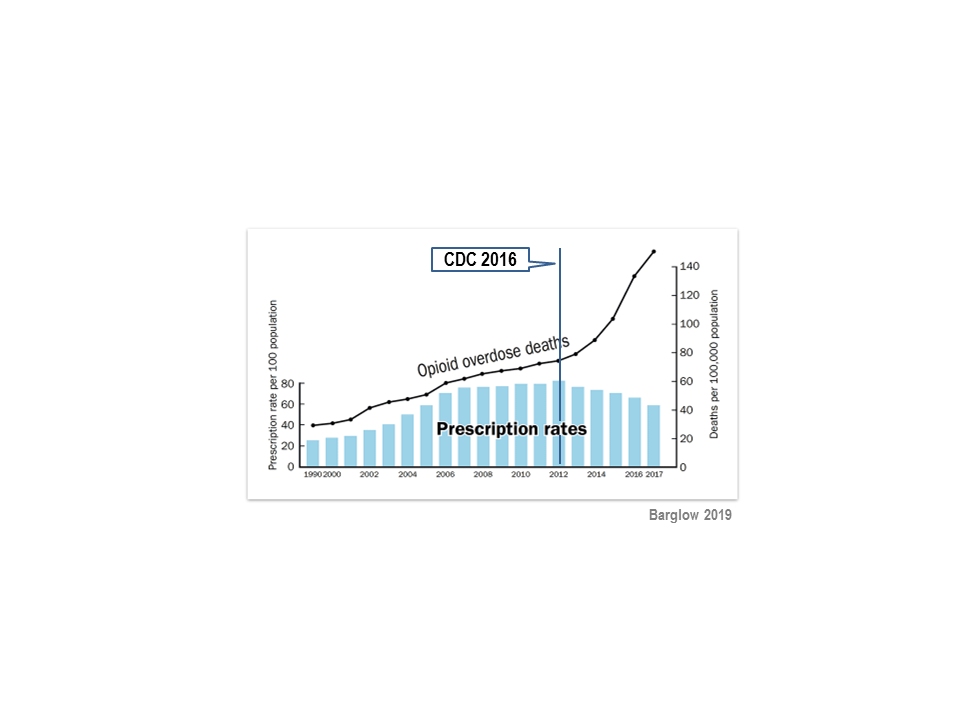
The included chart clearly demonstrates that OD’s went up dramatically, the line that noted when the CDC posted those guide lines is WRONG… it indicates 2012 when in fact it was 2016 – HOWEVER – 2012 was the peak of opiate Rxs being prescribed and the chart is correct that they dropped every year after 2012.
Apparently there are a few states who have passed so sort of law that is suppose to ensure prescribers that it is safer – less/no recourse for doing so, but I have asked many times that how can a state pass a law that will prevent the DEA from coming into state and use the Federal Controlled Substance Act to raid and shut down a prescriber’s practice and confiscate all his/her assets. But I can’t remember anyone presenting a valid argument that they can prevent the DEA from coming into a state.
The CDC published their opiate dosing guidelines in 2016 and in hindsight it now seems more like a trial balloon … they knew that they didn’t have the statutory authority to do it, but – what the hell – both the DEA and the VA wanted these guidelines and if no one challenged their legality in the courts… they could come back in a few years and claim that they had been grossly mis-applied and so they were going to revise them… at the same time that Congress is taking up new bills… that will codify those CDC opiate dosing guidelines… and maybe even just made the new law to will automatically adopt any changes the CDC makes to those guidelines in the future.
Never mind that those MME conversion programs was developed using SINGLE DOSES on acute pain pts and really little/no application to properly dosing intractable chronic pain pts… Never mind that there is such a thing as CYP-450 enzyme opiate metabolism and it is a proven fact that there is about 5-6 levels of speed of opiate metabolism in the body from poor to ultra fast. For century treating pts has been called the “practice of medicine”, but now we have the “cookbook formula” of treating pain.
Like all criminals, crooks, thieves and liars… they first some minor crimes at first and if they get by with it … they keep trying something BOLDER… they typically get to the point where after repeatedly getting by with criminal activity.. they try things that are more and more brazen…with bigger payoffs… the vast majority end up getting caught. But close to 50% of crimes remain unsolved and end up being cold cases…
Right now in the small town of Bardstown, KY there are three unsolved murders – one being a state trooper – after abt 5 yrs.
The DEA started 5 yrs ago reducing the pharma industry’s production quota that they are now producing abt 50% less now and they are already putting out press releases that they are going to reduce it farther in 2021. maybe they will ignore these state laws because at the rate they are going in reducing pharma production quota by 2025-2026 there is going to be very little legal opiate produced.
The DEA won’t have to raid any more prescribers’ practices or pharmacies… the prescribers can write all the opiates that they wish… because there were be little/no opiates in the pharma distribution system. When the Pharmacist tells a pt that they are “out of stock” … he/she will probably being telling you the truth.
The DEA won’t have to worry about the drug wholesalers shipping suspiciously large orders of opiates to pharmacies.. after all we have some 60,000 pharmacies… that is a lot for the DEA to stay on top of…
DEA has already lost their “cash cow” of Marijuana and if they can just move on to declaring Kratom has no valid medical value and will reclassified it as a C-I – which the control substance act only give that authority to our Surgeon General… and they will then be able to start chasing the diversion/abuse of Suboxone type products…. After all it is a C-III controlled substance so all the data as to the products are sold to via a wholesaler, the pharmacy that dispenses it and the doc who prescribed it … via the state’s PDMP. They will just have to create a new category of prescribers and vendors to go after… and it doing so they will be meeting the primary goal/function of all bureaucracies … to perpetuate and grow the bureaucracy.
The CDC reports drug OD deaths.. they don’t bother delineating between legally prescribed meds, illegal meds and use/abuse of NSAID’s that it is claimed kill 15,000/yr… and we may never know how many of those deaths labeled at a DRUG OD… is in fact a SUICIDE – or as they would rather have it referred to as “death of despair”.
Besides, most of those who die from something… are most likely “high cost medical care”… treating their mental health of addiction with medications, or putting them in jail/prison, or chronic painers are believed that they will never be part of a productive manner of our society – pays taxes – so they have been classified as a “taker” and will never again be a “maker” in our society.
Like this:
Like Loading...
Filed under: General Problems | 4 Comments »


















 Joe Biden claims that he is going to only raise taxes on people with over $400,000 .. apparently to help pay for his proposed “medicare for all”…
Joe Biden claims that he is going to only raise taxes on people with over $400,000 .. apparently to help pay for his proposed “medicare for all”… 





