“The moral test of a government is how it treats those who are at the dawn of life, the children; those who are in the twilight of life, the aged; and those who are in the shadow of life, the sick and the needy, and the handicapped.” – Hubert Humphrey
passionate pachyderms
Pharmacist Steve steve@steveariens.com 502.938.2414
We, the undersigned, stand as a unified community of stakeholders and key opinion leaders deeply concerned about forced opioid tapering in patients receiving long-term prescription opioid therapy for chronic pain. This is a large-scale humanitarian issue. Our specific concerns involve:
rapid, forced opioid tapering among outpatients;
mandated opioid tapers that require aggressive opioid dose reductions over a defined period, even when that period is an extended one.
Opioid tapering guidelines were created, in part, to decrease harm to patients resulting from high-dose opioid therapy for chronic pain. However, countless “legacy patients” with chronic pain who were progressively escalated to high opioid doses, often over many years, now face additional and very serious risks resulting from rapid tapering or related policies that mandate extreme dose reductions that are aggressive and unrealistic.
Rapid forced tapering can destabilize these patients, precipitating severe opioid withdrawal accompanied by worsening pain and profound loss of function. To escape the resultant suffering, some patients may seek relief from illicit (and inherently more dangerous) sources of opioids, whereas others may become acutely suicidal. Regardless of one’s view on the advisability of high-dose opioid therapy, every thoughtful clinician recognizes rapid tapering as a genuine threat to a large number of patients who are often medically complex and vulnerable. Indeed, even slower tapers should include realistic, patient-centered goals that are achievable and account for individual patient factors.
New and grave risks now exist because of forced opioid tapering: an alarming increase in reports of patient suffering and suicides within and outside of the Veterans Affairs Healthcare System in the United States.
Reports suggest that forced tapering is also occurring in patients on opioid doses below the Centers for Disease Control and Prevention Opioid Guideline threshold of 90 morphine equivalent daily dose. These patients too are at risk of harm from overly aggressive tapering.
Patients on legacy opioid prescriptions require different considerations and careful attention to the methods by which opioid tapers might be considered and implemented. Currently, no data exist to support forced, community-based opioid tapering to drastically low levels without exposing patients to potentially life-threatening harms. Existing data that support rapid reductions of opioid doses—often to zero—were conducted in highly structured, supportive, interdisciplinary, inpatient settings or “detox” programs in which medications and other approaches were used to minimize the symptoms of withdrawal. These data do not inform community-based opioid tapering. Currently, nonconsensual tapering policies are being enacted throughout the country without careful systems that attend to patient safety. The methods by which a taper is conducted matter greatly.
We therefore call for an urgent review of mandated opioid tapering policies for outpatients at every level of health care—including prescribing, pharmacy, and insurance policies—and across borders, to minimize the iatrogenic harm that ensues from aggressive opioid tapering policies and practices.
Almost 18 million Americans are currently taking long-term prescription opioids. We ask the Department of Health and Human Services to consider the following to mitigate harms in this special, at-risk population:
Enact policies that prohibit or minimize rapid, forced opioid tapering in outpatients taking legacy opioid prescriptions (this includes prescribers and health care organizations, pharmacies, and insurance payors).
Provide compassionate systems for opioid tapering, if indicated; that includes careful selection, patient-centered methods, close monitoring, triaging of adverse events, and realistic end-dose goals that are evidence-based and derived from applicable outpatient tapering data.
Convene patient advisory boards at all levels of decision-making to ensure that patient-centered systems are developed and patient rights are protected within the context of pain care.
Require inclusion of pain management specialists at every level of decision-making about future opioid policies and guidelines.
In standing as a unified community of concerned scientists, experts, citizens, and leaders of pain organizations in our respective countries, we call for the development and implementation of policies that are humane, compassionate, patient-centered, and evidence-based in order to minimize iatrogenic harms and protect patients taking long-term prescription opioids.
Sen. Caleb Rowden is interviewed by liberty guru Gary Nolan. Caleb explains that the new reason for passing a 2019 PDMP bill is keep the St. Louis County PDMP from passing your personal information on to the federal government, which could use it to infringe on your right to bear arms. What else could he say? All the facts indicate that PDMPs simply aren’t working in the 49 other states that already have them. But the new “reason” holds no water, since the provisions in the statewide PDMP bill are not legally binding to other states or the federal government.
When the U.S. Centers for Disease Control and Prevention published its opioid prescribing guidelines in 2016, the American Medical Association worried about “unintended consequences,” including “the potential effects of strict dosage and duration limits on patient care.” Since then those consequences, including needless suffering, despair, and suicides caused by involuntary dose reductions and patient abandonment, have become painfully clear, as the authors of the guidelines finally acknowledged last week.
Writing in The New England Journal of Medicine, the guidelines’ authors said their advice has been “misimplemented.” But they took no responsibility for the unintended yet foreseeable results of their recommendations, and their warning may be too little, too late for the innocent victims of the government’s cruelly misguided fight against opioid-related deaths, the vast majority of which involve illicit drugs rather than prescription analgesics.
The NEJM article echoed an April 10 letter in which CDC Director Robert Redfield emphasized that his agency “does not endorse mandated or abrupt dose reduction or discontinuation, as these actions can result in patient harm.” Redfield was responding to a March 6 letter in which more than 300 health professionals and addiction specialists, including three former drug czars, expressed concern about the fallout from the CDC’s guidelines.
The letter included reports from hundreds of patients around the country who have suffered as a result of policies and practices based on the guidelines. “Undertreated pain is killing me!” wrote a Syracuse, New York, patient with osteoarthritis and tethered spinal cord syndrome. “You don’t know me, you don’t walk in my shoes, you don’t have my nerve damage, and you don’t have to live with the thought of will today be the day that I kill myself because I can’t take the pain anymore,” said a patient in Washington, D.C.
“This policy is just cruel,” wrote a woman in Albany, California. “Every patient is an individual and should be treated with care and respect so they can live a functional life—and not given inappropriate or ineffective medication.”
When a document is as widely misconstrued as the CDC’s guidelines have been—by insurers, regulators, legislators, pharmacists, and law enforcement agencies as well as clinicians—it is fair to ask how the authors left themselves open to misinterpretation. According to the guidelines, doctors “should avoid increasing dosage” above 90 morphine milligram equivalents (MME) per day “or carefully justify a decision to titrate dosage” above that level.
The implication is that doses of 90 MME or more per day are rarely, if ever, medically justified. It is hardly a stretch for physicians with patients who exceed this arbitrary threshold, including patients who have been functioning well on high doses for years, to worry that they will be perceived as practicing outside the bounds of proper medical care.
Given the scrutiny that regulators and law enforcement agencies have been applying to doctors in recent years, prescribing practices portrayed as extreme and dubious by the CDC are apt to attract unwelcome attention that could jeopardize a physician’s livelihood and liberty. In this context, forced tapering and abandonment were predictable outcomes, even though the CDC guidelines say doctors should reduce doses only when the risks outweigh the benefits and describe the process as collaborative and consensual.
“We all warned of this outcome when the ‘guidelines’ were issued,” says Mark Ibsen, an emergency medicine physician in Helena, Montana. “The CDC guidelines have been as harmful as predicted, and the silence over three years has been criminal.”
Patrice Harris, the AMA’s president-elect, worries that “the guidelines have been misapplied so widely that it will be a challenge to undo the damage.” Lynn Webster, a former president of the American Academy of Pain Medicine, is even less optimistic.
“I am afraid that cultural attitudes, fears, misinformation, and prejudices are baked into the system,” Webster says. “It may take a generation before a more sensible and compassionate approach to treating people in pain with opioids is established.”
Can telemedicine replace a traditional visit to the doctor? Dr. Mike doesn’t think so. He’s worried that the drive for profits will take center stage, shoving proper healthcare to the rear.
Following is a transcript of his remarks in the video:
To summarize, a study was published in the Journal of Pediatrics that showed children who had a consultation with a telemedicine doctor had a much higher rate for a prescription of antibiotics than if they were to be seen at a primary care office like my own. Now why is this problematic? Well, I’ll tell you. The huge majority of respiratory tract infections, basically colds, don’t require antibiotics. This is because antibiotics don’t work on viruses. You’ve heard me say this literally a million times.
Why is that such a big deal? They got more antibiotics. Doesn’t that mean they got better care? No, not necessarily. In fact, definitely not. Respiratory tract infections by the huge majority are caused by a virus, meaning that they don’t require an antibiotic. Antibiotics only work on bacteria, and I’ll briefly run through the list of why over-prescribing antibiotics is bad.
One, cost. You shouldn’t be paying for a medicine you don’t need. Two, antibiotics are not benign medications. They have true adverse events: diarrhea — like we talked about at the opening — rashes, allergic reactions, your throat closing up, and finally resistance. That superbug I’m always talking about, about that bacteria that can get into your system where antibiotics can’t even fix it, that’s scary stuff.
I understand why telemedicine is so popular. I mean us, millennials, we treasure convenience almost above all else. We want to save time. We may be traveling. We don’t have access to a doctor. The cost is less when we use a telemedicine consultation, as opposed to going to a doctor’s office.
But it truly is alarming to hear that telemedicine may be hurting the outcomes for these people who want better convenience, who want more access for lower costs. I think the reason why telemedicine doctors are over-prescribing antibiotics are as follows. First and foremost, there is usually no relationship with the doctor and the patient.
Now, if one of my patients comes to see me, I know what they’re like. I know if they’re really sensitive, that if they have a stuffy nose they can act very dramatic. Or, I have some patients that if I see they have some pain, they have such a high pain tolerance that I really do worry and get an X-ray early on. But if you don’t have that sort of doctor-patient relationship, you may come to an incorrect conclusion.
Second, if you’re doing a telephone consultation, there is no physical exam. Think about that for a baby. If a mother calls and says her child is fussy and has a fever, it’s hard to decide whether it’s viral or bacterial without a proper physical exam. I mean, you need to look in that baby’s ear. But without that physical exam, you may be practicing what’s known as C.Y.A. Medicine, cover-your-butt medicine. That’s when you’re so worried about being sued by a patient, by them becoming worse and you not treating them with antibiotics, that you just over-prescribe antibiotics in the hopes of covering your butt.
Now I’ve seen this happen one too many times, even in primary care offices, so I can only imagine how much more often it’s happening in a telemedicine consultation where there’s no existing relationship and no proper physical exam done. It’s obvious that you’re not going to have great outcomes in this case.
One of the more concerning things that I’ve actually read in a study that was done in late 2018 was that doctors who practice telemedicine, who are generally just scattered throughout the country, those doctors had higher satisfaction rates and shorter visit times. And guess what doctors get compensated on? Shorter visit times and higher patient satisfaction scores. That’s the problem right there.
If doctors are more motivated to get you out the door and just keep you happy, they’re going to give you whatever it is that you want. Just because you want an antibiotic, it doesn’t mean that it’s the right treatment plan. Sometimes, the visit may need to take longer because the doctor should be educating you on why you don’t need an antibiotic, on what lifestyle things you can do to maybe speed up your recovery, and maybe to prevent you from having the same symptoms next time.
It’s kind of crazy to me as a doctor that by doing the wrong thing, over-prescribing antibiotics, you can have higher patient satisfaction and shorter visit times. That’s wild. As a young doctor, it really gets me excited when technology and healthcare combine. So when I hear the story about telemedicine not giving quality care to patients, it truly upsets me because I see how advantageous telemedicine can be. You can have lower costs and better access to care. You can have consultations with specialists who may be in a totally different city than you, but who can give you really great advice. It’s just in this case the standards of care are not being maintained. We need to hold telemedicine docs accountable for over-prescription of medications, change the incentive system so that we don’t just focus on patient satisfaction and shorter visit times, but instead focus on quality medicine, in addition to those factors.
I’m excited for the future of telemedicine and frankly, you should be too. Telemedicine antibiotics seem to be struggling. But here’s another instance where telemedicine fell short. Check out my video here. Click it.
Mikhail Varshavski, DO, (better known on social media as “Doctor Mike”) is a board-certified family medicine physician at the Atlantic Health System’s Overlook Medical Center in Summit, New Jersey. His YouTube channel educates over 3 million subscribers with two weekly shows covering everything from trending medical stories, to health myths, to reaction videos critiquing popular medical TV dramas. His goal is to expose medical misinformation and increase the health literacy of young adults.
Specifically, I will never forget Senator Bob Casey sending me a form letter about immigration when I sent him a letter, detailing my hospital stay from hell. Great public servant, Bob. He wears flannel when he visits my hometown. You know, so he can dupe the folks at the Shop ‘n Save into thinking he is like them.
The ACLU National repeatedly refused to help a single incurable painful disease patient. It was “above their pay grade”. Or something.
No lawyer would take a case. Not sexy enough.
Reporters, by and large, jeered at us when we asked for corrections.
Only a very few journalists were brave enough to report real facts, truth, real data.
Daniel Horowitz of Conservative Review was one of those brave few. His series on the so called opioid crisis was superb. He seemed a decent person to those of us who asked questions.
But their few voices were always drowned out by the relentless hammering of The Machine.
There was plainly and obviously something wrong here.
When this concern was voiced, the person voicing it was quickly ridiculed and dubbed a “tin foil hatter”, shown quickly to stage left and told to leave.
Black holed. Even by so-called “pain” groups. What a joke.
I am here to announce we are vindicated.
There indeed is something wrong.
Something damnable.
Something so violating and outrageous, one will scarcely believe it’s true.
But it is.
It’s real. It’s happening. It’s ongoing as I type.
I wish I could say that hitting publish on this piece will end it.
It won’t. Because evil never goes away that easily. Look at the world.
But at least YOU WILL KNOW WHY.
I preface this piece with a truth, somewhat of a disclaimer.
By saying that we real advocates work in the red. No, I am not asking for money. I am telling you that we are real.
Despite what you may have been breathlessly told otherwise. Told by those so called advocates that stay a quarter step behind drama, have a screenshot convenient for every situation, and who work “tirelessly” doing absolutely nothing except keeping good people riled every day on social media.
Do they do anything else but that? No. Simply, no. I suppose they do work tirelessly, just not for you and not for painful disease patient rights.
Self aggrandizement and humble braggadacio via tweet or post is not working for patient rights.
It’s beyond the pale that our own government thinks nothing of using addicts in a “quid pro quo” of their own desperation and paying their own senatorial/representative staffers to pose as “patients with sick wives” to infiltrate painful patient groups and report back all they see and hear.
We don’t get paid for the long hours, nights, and weekends we spend digging up all this… horror. Unsnarling it so we can show you.
It’s… really just that simple.
There will be many damnable, filthy lies, many horrible character assassinations published, texted, whispered regarding me, regarding others, specifically Lauren Deluca and Shasta Rayne Harner, the ones who brought this unbelievable information to me, we all were shocked …who have risked everything, risked it ALL to bring this information to YOU.
Do you think this is not deadly serious? This isn’t a movie, a book, a video game. This is real life, with real people. People they do not give one tiny shred of care about. Because you are watching is the only reason we are breathing. Keep watching.
The government operatives peppering our patient movement who attack advocates, the ones masked as patients… it’s truly unbelievable. The backpedaling, lies, false victimhood, stealing of credit, and backstabbing has begun already in earnest. It is spinning higher and higher.
Please use critical thinking.
That is all I have ever asked of you — as you well know if you have been and are my wonderful follower all this time. I do care about you. I do.
Use your intelligent, common sense, critical thought.
If you are here for drama’s sake?
To hell with you.
Shame on you!
Go back to your pit. I know who you really are. And better yet — who you really aren’t. I have never done a single thing in regards to incurable painful disease patients that would make me ashamed, because I have been fighting for them since I became one and found out my government wanted to kill me. I have never lied or entered a back deal for powerful influence or money. I have never struck a deal to harrass an advocate for money or influence or to be “liked”.
When all this is said and done, I will retreat to my corner of Medium and resume my writing that 20 odd people may read or share. My dream of starting an advocacy group for rare painful diseases has been put on hold because of trolls, likely fake patients.
I am not a CIAAG employee or board member. I am merely a person with which Lauren Deluca and Shasta Rayne Harner share a mutual respect of shared interests and goals, who they approached to help with writing and research.
No one is being paid. Not on our side anyway.
Again- I will gladly share my tax forms this year with anyone who doubts me. It had 0 dollars next to my name for income. Lucky for me, my husband has a good job and supports me financially. I hate not working and I miss it. Advocacy work doesn’t pay bills. Being a turncoat, informant, and online stalker pays bills. Ask them. Have you ever seen them, their faces, in real life? Their taxes, the forms, in real life?
My goal also is to open the door and turn on the lights so the coyotes hiding in the corners and the roaches creeping under the tables come out, desperately trying to flee.
Good advocates have people “assigned” to them, to befriend them or to harass them endlessly.
It’s horrible and also unfortunate to find those you thought were real friends… weren’t. They only “liked” you because they were paid or told to befriend you by evil, corrupt, envious people in attempts to get information.
The real patients will finally know the truth. What was done to them and why. This is for you.
Rats in a Cage
You must check your politics here. There is NO room for partisan politics. Any reference herein to a politician is simply to point out what he/she did, or make fun of them, not to go on a personal belief tangent.
Every one of them suck. They all knew. All of them.
The United States Government, through the CDC, has implemented a massive clinical trial- a population based study, through the creation of the Centers for Disease Control’s 2016 Guidelines for Opioid Prescribing for Treatment of Chronic Non Cancer Pain. The evil plot originated in Washington State. It was hatched to flow through and be included in the ACA, and everything since that awful law was passed marched the country toward this end. The Guidelines were a conduit.
This is real and has been admitted to by our United States Congressional and Senatorial offices.
The PR machine has ran non stop since, spinning desperately to distract you and dismiss what I am telling you, to hopefully deflect blame away from politicians.
They are terrified you will not vote for them next year and likely will throw them out.
What?
What do I mean by this?
The Government (and others) wanted to study pain patients who were using opioids and they wanted to take them off their opioids.
They knew that, well…people like being pain free (and able to work- though they won’t admit that). They wouldn’t sign up willingly for that and they needed a huge pool of people to study.
What better way to get one than to push through horrendous stipulations such as the CDC guidelines… then the National Pain Strategy and…
Watch what happens and record it all. Use it for preventative health, study of disease, and a kind of “pre crime” profiling too.
This is a much faster, easier way… without getting a single signature of consent- that pesky damn informed consent.
That stupid HIPAA. The smoke and mirrors law that no one ever enforces outside a few obvious placaters.
Wanted everyone off opioids to study what happens — and also because they straight up think anyone who uses opioids is an addict, The End. We all are losers who want to get high all day and waste their (insert faux indignation) money.
They knew they could not get volunteers. So instead? They forced a horrific situation upon THE ENTIRE NATION.
That is how much they value each and every person in the vast American public. We who vote for, rally for, and pay for.
Because it doesn’t matter to them. It did not and will not affect their health or their care. They made damn sure of that in the ACA.
As I said in my previous pieces leading up to this one, socialism never affects the self appointed elites. Their personal care and family’s care was never affected. They never writhed in pain.
Pretty sweet, really kind of our public servants, the ones we pay.
Obama passed the actual laws for them (sorry, guys, but he did) and then they got all their ducks in a row. The previous fellas sure helped, make no mistake.
“Keep Smilin’ Boys! They will never figure it out!” {Getty Images fair use}
The ACA (also known as the worst piece of s*** legislation in American History- aka “the insurer handout”) gave broad powers to HHS. To insurers. To private corps, like Appriss.
Well, it’s okay. No one read it. How were they supposed to know, right??? I mean, that excuse they have used for so many things…
Of course, no one said a damn word. They never did about a thing while Obama was President, let’s be real here.
Part and parcel why this plan had to happen during the Obama administration.
This would never squeak by any other White House — even Bill! The media and every person in Congress would be on them like starved wolverines on an injured doe.
HHS never enjoyed such powers as these before. George W. “Mistakes were made” Bush and Darth Cheney had nothing on this… but then again, Cheney shot a man while hunting and walked free.
After he made the man he shot apologize to him. Because, like, manners.
HHS was given powers under the ACA, mostly under Title IV, like:
Creating the powerful, hidden 15 person “National Prevention, Health Promotion, Public Health Council”.
Creating the “Center for Medicare and Medicaid Innovation” (with their little subgroup, ‘Institute of Healthcare Improvement’- a bean counter group interested in one thing — cutting costs, lives be damned. How Karl Marx of them!)
Strategized “Healthy People 2010” a group with faux smiles and one size fits all (socialist) mentality of treatment, grouping all under one treatment model-theirs.
Creation/Funding the infamous (to the very few advocates who have found this thing and read it) “Living Well with Chronic Illness” e-book/guide through the nefarious “Institute of Medicine” incredibly renamed the “Health and Medicine Division” on March 16, 2016, the same day as the release of the CDC Guidelines. I’m sure that was one of those fantastic coincidences.This publication is not to be confused with the book by author Joanna Charnes that has been mysteriously shoved up HIGH in Google search the past two days. We will come back to this document — note it recommends studying all groups in the USA. Well, except white males. Everyone else though! Hitler 2.0 up in here!
Developing the “Health in All Policies” approach with CDC, National Prevention Strategy — the government-level way of saying to every single government agency: “Remember in grade school, we all had to use the sh**ty scissors? No one was allowed to bring in a pair? If you were left hand, you got green handles, right hand, blue? Well, this is our scissors policy. Every last one of you is implementing this thing, whether you wanna or not. No crybabies,” announced at a meet of the “National Prevention Council” a snug group of leaders from every single agency in our thoughtful government (sec. 4001 in ACA)- through the Surgeon General’s Agency. His tweets make so much sense through this lens. How dare he!
Since Healthy People 2010, the Institute of Medicine (not whatever that bland, inoffensive name they imagined themselves to be the day the Guidelines they directly caused came out) recommended another initiative — “Healthy People 2020–2030”. Basically an every decade thing.
HHS has given the green light to the Office of Surgeon General that “Health in All Agencies” (HiaA) be used to craft HP ‘30.
To make sure the goals of these programs created in 2010/2011 were actually being met, of course a surveillance system had to be put into place.
Later on, they could “hook” EHRs into this system, already tailored to carrying electronic information, and call that the gateway. Appriss Gateway, in fact. In 2012 the Kentucky State legislature made a law called the Kentucky State Prescription State Monitoring Compact (not program — COMPACT). There are stakeholders and investors in this compact, with annual reports required and generated. Not a single one of those reports exists for public perusal, nor does even a list of its members exist for review. Requests have been blatantly ignored. Oh, and Appriss is located in Kentucky. Coincidence alert!
The surveillance system was firmly under the care of another congressman, Rep. Hal Rogers– R-KY- Apprissville, Prince of Pork himself. Sure, that is a great idea.
There was the HUGE question of consent, here.
They decided to completely sidestep consent by simply pretending it didn’t exist.
By pretending that a patient who signed a form at that office for their care at that office was somehow informed and understood what was happening and the myriad of ways his/her information would be viewed/bought/sold/studied as part of the PDMP programs.
Hell, the entire premise of what was occurring was already flagrantly so outrageous.
This was nothing. A drip of candle wax on a sh**cake with ten layers.
So, what do we have thus far?
When the ACA was conceived, these people put their plan into play. These innocent sounding orgs were all created under the umbrella of HHS. Powerful men and women came in with an agenda, a very twisted agenda, under the banner of “health and wellness”.
What it really was — eugenics and population engineering, a real time study of genetics and disease markers/ indicators.
To be clear, there is nothing wrong with science. Nothing wrong with study of disease. Nothing wrong with promotion of health and wellness.
It’s all monstrous when it is done to unwitting people. It’s a horror movie when people are used as lab rats and guinea pigs in experiments without their consent or knowledge. It is a crime against humanity to withhold pain medication, “to see” what happens.
Especially when assisted suicide is one of those “whats” on the table — as it is in 8 states now, NJ the latest to topple.
It’s called “gaslighting” in psychology when a person attempts to convince another person a valid, lived experience didn’t actually happen with manipulation and seeds of doubt.
Did the government learn absolutely nothing since Tuskegee?
Since the 70’s with their twisted psych personality shattering garbage goings-on?
Perhaps they did …and this is the result.
I observed before that evil always reinvents itself, improving upon the mistakes of its predecessors.
This is happening today, right now. This is not a “theory” of what happened.
We have the government with stakeholders in insurance and other private entities — but mostly insurance — who met up with physicians and said:
You know? We think these people who take opioids are just a bunch of losers who sit at home getting high all day with our disability and worker’s compensation money, while we pay it every month. We need to get these lazy jerks off their a***s and this is how we are gonna do it. And furthermore, this whole pain meds thing is ridiculous. We don’t need to be paying for pain medication period for all these people. They need to suck it up, buttercup, like their grandmas did, and figure it out themselves. I mean, of course, you know, we will be making sure we have enough for ourselves, but those people need to learn who their betters are somehow, but while we are pushing all this equality s**t.
Here’s how. Make it happen.
Do you even have a clue how much money we will make, oops, I mean, save?
Oregon has it right all along, letting people off themselves. In fact, we sure would LOVE to know how many people would off themselves if they got their pain pills taken away forever. Because that is our national, in fact, World, goal. In both respects. Let’s watch there first. Because we don’t have a solid grasp on these random suicides. CDC isn’t tracking those well enough.
Where is Kolodny in all this? Everyone knows I think Andrew could probably pass the entrance exam for kindergarten. After that, it may get dicey.
I am almost fully certain that Andrew Kolodny will be sacrificed by his handlers in this thing, and in the coming weeks, many incurable painful disease patients will see a vindication the likes of which hasn’t been seen since the news came in they caught Ted Bundy.
Unfortunate, in there is no way on earth this thing could have been machinated by the likes of him, sorry. Anyone with a whit of sense would know that.
However, you reap what you sow, Andrew. Hey, I don’t even think you are smart enough to have even come up with the names of some of these groups, if that is any consolation. I am just an incurable painful disease patient though, so you hold me in the least esteem — and you have spent the last almost 15 years attempting to convince America I am a drug addict who drools when she speaks and is unable to form coherent thoughts. My words are worthless to you.
Who would have ever believed there used to be a time when Roger Chou and Jane Ballentyne thought that painful disease patients could have long term opioids, that it was okay?
They did think this was okay — in 2009. It is simply amazing how all one believes can change like that, because of a “promise” or something else…
The biggest trigger that caused this to be green-lit, no passing go, was the Baby Boomers. Yes, I know. I have those feelings, too, sometimes. I was raised by Boomers.
The Baby Boomers are getting old, though.
The first ones started knocking on Big Government’s door for their money — the money they paid into Social Security and all that jazz in June 2012.
Well, why not? It is not entitlement when you paid your whole life into this system.The Boomers by and large did. They worked.
The Washington greed factory foresaw all their perks, expense accounts, lavish spending going into an endless dark vat that is the Baby Boomers when the realization struck them these few claims were the extreme tip of a monster iceberg with a voracious appetite.
What better way to shut off that faucet? Taking away their pain relief, demonizing opioids, making the senior baby boomers feel like addicts for taking an opioid after years of stability taking one… or not allowing any when the time arrived that one needed it.
Less opioids= pain filled, shorter life expectancy/possible suicide= less benefits paid. More money stays in the life insurance account in DC. Of course, not the Boomers lucky enough to be in Congress, but everyone else.
Health, “Wellness”, Prescribing
The race was then on, the ACA was signed into law. The plan began to hatch all its subplots and subplans.
Stakeholder groups got into the action, and here is where crony capitalism is showcased and shines.
Abt Associates was contracted by the government to help them socially engineer the country into thinking opioids were horrible, filthy things. That anyone who used opioid therapy was a drug seeking addict. That any doctor who wrote a prescription was a “drug dealer in a white coat”. DEA suddenly was off the hook for their monstrous failure in keeping illegal Chinese fentanyl out of our country, as physicians were blamed for the first time in history for the deaths of addicts, even in the face of science.
2013 Asset Forfeiture- Starting in CA, laws were weaponized against physicians, and the DEA used this liberally to seize assets of doctors who they arbitrarily decided to arrest — after they used the (now weaponized) PDMPs (prescription drug monitoring programs). The one-two punch frightened doctors into virtually no prescribing of opioids.
2015-California’s Death Certificate Project is worst of all. A classic case of scare tactics via legislation, the government combs through old death certificates looking for “inappropriate prescribing practices” that “may have contributed to demise”. A sheer fright tactic to keep docs from prescribing — all in the name of this study!! There is no opioid crisis. Just their study! How many physicians are or have been arrested and/ or jailed and/or fined all in the name of this study?!
Not to mention the myriad of different ways and means of study done through the PDMPs themselves — the aforementioned hyperlink under Dr. Kreiner is to one of those ACA hatchlings that was thrown to the VA, “to assess the impact of the Veterans Access, Choice and Accountability Act of 2014 (VCA) on appropriateness of opioid therapy”.
Not only were the surveillance systems mass implemented without a single signature of informed consent, but the systems themselves were used in countless ways to extract reams of sensitive data from unsuspecting patients and sell it to the highest bidder on the healthcare market, as well as “study” in slanted and biased ways to forward this agenda.
As previously mentioned, Rep. Hal Rogers is the Congressional front man on this. Gubernatorial appointments were made to the KY Prescription Drug Monitoring Compact, a self serving, self enriching stakeholder group slipped through legislation.
We have no way of knowing just what data and where all this information went, because these agencies hide behind so-called “proprietary” algorithms and will not disclose their data fields.
A violation of HIPAA, privacy, human and civil rights that is incalcuble.
Healthy People2010 was implemented with bright splashy graphics on their website. And we all fall for it every time they pull this crap. I have. We just do.
They do these things and invite public commentary — not because what we say is going to actually shape any policies.
Because we are all part of the study now, and they want us to participate in it.
It is fully Orwell’s world.
They file away the comments and move on to tweak the process based on the feedback- tweak it in a way that we won’t notice what we complained about previously.
It is not us shaping the policy. It is them shaping us through the policy.
HHS does this every time with their TaskForce Public Dockets. They post these for patients, not because they want our thoughtful comments and will listen to what we have to say.
They do this because they are required to do so by the ACA, they have to check off the box and show they received public feedback. No more. Hence why we feel ignored.
Because we are! They have absolutely zero interest in anything we have to say. What we think has nothing to do with what they are doing and will shape none of it.
This ties into the “advocate” clinicians on social media. Many patients believe that the clinicians on social media who are surveying them and studying them are on “their side”.
No.
Use of Social Media as Study Device/ Social Engineering Mechanism
The incurable painful disease patient communities exploded online in the wake of the implementation of the government’s scheme.
This was exactly what the government wanted to happen. They knew that people would be easy to study, manipulate, and also they could use the internet to their advantage socially to a large scale to push through their agenda through social engineering.
HHS and NIH, along with several college and university research departments immediately dispatched a multitude of their “finest”.
To pose as patients, troll agitators, patient sympathizers, advocates, leaders of movements… it is so thick in the incurable painful disease patient advocate movement at this point on social media between several different vested interest groups and the government, that one would be more likely to fall in with a faux advocate or faux patient than one would with a genuinely sick person in need of aid. It’s that disgustingly bad. Add in big pharma and their disinfo agents, and it truly is a hot mess.
Not to mention the junkies and the hypochondriacs that are always attracted to these groups. The junkies were immediately pressed into service. They were put to work as trolls and agitators. Paid in trade or cash to actively go after genuine leaders and effective opioid crisis advocates.
They would troll, agitate, and do as much as they could to get that person banned or deactivated off social media so their voice was silent and doing no damage to the government’s work.
These people would infiltrate every group they could, take screenshots of conversations, cause chaos in their wake wherever they went, and spent all their time on social media pretending to do good while being the very worst of human beings. It’s quite gross, the stunning hypocrisy. Lying about themselves and their lives to ingratiate as closely as they could to as many as they could. Blocking these people was like a death in the family to them. They carried on as though it was.
Many are active at this moment doing this very thing. People love drama. This won’t ever stop. The drama they provide keeps them popular.
The others were far worse.
Researchers swarmed in. Some were pretty open about what they were doing, however, patients mistook that openness to mean that person was working for the patients and helping them “gain their meds back”. Nothing could be further from the truth. These researchers had carte blanche to say whatever they had to. They were to gain the trust of patients so the patients would provide information to them — in the forms of surveys, stories, and infographics. Or better, messages in private groups that would provide a rich tapestry of accentuation to the research papers being written.
This proved to be surprisingly easy. Patients were desperate for someone to validate their experiences, especially an authority figure, someone who was a doctor or professional, and these horrible people played them like a fiddle.
Advocacy statisticians, NIH analysts, physicians from the beginning days in Washington State…so many people in the know would play both ends against the middle, dashing away to write it up and submit their pieces to JAMA, NEJM, and the like, or to provide to other physicians and psychiatrists who needed the information to plug holes in their “research”.
Patients were none the wiser.
ACA 4305 Advancing Research and Treatment for Pain Care Management
The part of the ACA that actually directly addresses pain, pain care and treatment is so short and vague as to render this entire topic rote and meaningless.
The only part of this that would raise any eyebrows to anyone is the little nugget buried in paragraph 2 under subsection (a) under 409J of 4305 says this, “ANNUAL RECOMMENDATIONS. — Not less than annually, the Pain Consortium, in consultation with the Division of Pro- gram Coordination, Planning, and Strategic Initiatives, shall develop and submit to the Director of NIH recommendations on appropriate pain research initiatives that could be under- taken with funds reserved under section 402A(c)(1) for the Common Fund or otherwise available for such initiatives.”
The NIH Common Fund has a person or two masquerading as “advocates” on social media networks. It’s interesting to see the interactions being made with these people, simply because of the shark like social climber personalities known behind the profiles. With the Common Fund funding set up as such and desperation of people for money for their psychosocial projects, one has to wonder where the intersection lies? There is no shame, apparently.
The 6 Building Blocks
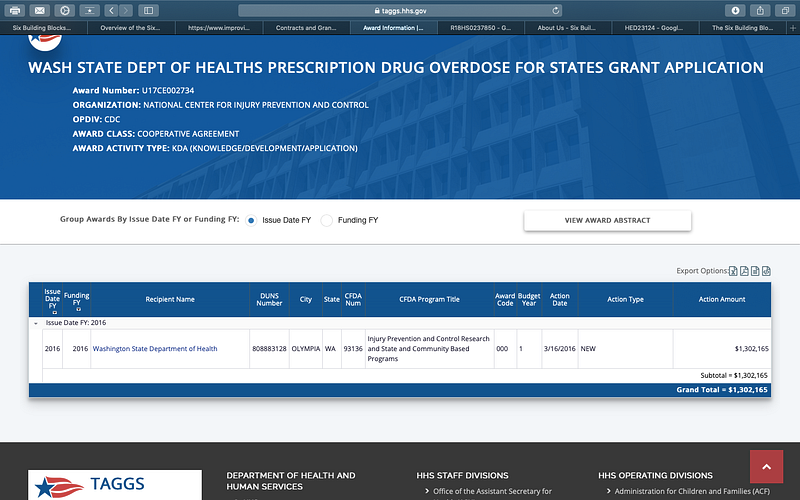
The day of the CDC guidelines were issued, HHS released grant money to the states for the creation of the 6 Building Blocks programs the very next day, March 16, 2016. Of course, this originates in Washington State U and is being sold as a program to help facilitate patient centered care for the complex patient who is on long term opioid therapy. And our friends from Abt Associates are here! Surely this program is in the patient’s best interest.
screencap of grant showing it was sent 3/16/2016- day after CDC Guidelines
The Definition of Bravery
The textbook definition of bravery is “the quality or state of having or showing mental or moral strength to face danger, fear, or difficulty.”
I have heard many patients and advocates carelessly say they would do many things… XYZ… if they found out what the “real” story was behind the CDC guidelines.
Well, here is your chance to prove it. I am telling you the story, the truth, and will you do what you have told me all this time?
Jayne Flanders is the co-founder of CIAAG. She is a beautiful, medically fragile young woman with brown hair and a shy smile. Has been with Lauren Deluca since day one, helping her build the little advocacy group from nothing. She has many incurable painful diseases, mostly genetic, and to hear of what she deals with daily makes my heart hurt. Ehlers Danlos Syndrome, Chiari malformation, Hyperadrenergic POTS, are but a few… and yet she works hard at home on this group, often from her bedside, as she is relatively bed bound.
She does all web design, social media content, organization of the web content and analyzing of the data. She works with Lauren Deluca of CIAAG on strategy and all decisions are made together.
Lauren Deluca and Shasta Rayne Harner, two painful disease patients, discovered everything I told you. Two disabled women.
After they discussed it with Jayne Flanders, another disabled woman, they brought it to me, yet another painful disease patient and woman they trusted implicitly.
Then they took it to Washington, D.C. to tell Congress they knew what they were doing.
To tell them to stop.
To tell them enough is enough.
How many more have to die to end the hellish agony their lives had become?! And all for… a study? To save money? Because extremely rich people were greedy and believed a lie?
Imagine two small women walking into Congress and saying what I just told you… right now.
That is what they did.
Because to do what they did… takes courage the likes of which there just isn’t very much of these days.
With courage and determination, they took their research and saw through their task to their goal.
The United States of America owes them a deep and enormous debt of gratitude.
Downloads for all to take to their physician, to hand out, et al… are available for free on CIAAGwww.ciaag.net
Now is the time to show solidarity as we unite. Our physicians need this. Our pharmacists need this. How dare they perpetuate this on a free society! Please spread this far and wide!
Use the hashtag #ViolationofANation to get their attention and let them know you know! Get it trending!
I will keep you all up to date on this profile as developments are forthcoming.
Heather Wargo is a Medium Top Writer in Government, Politics, Health, and Social Media. She is a freelance writer and advocate for incurable painful disease patients and physicians affected by governmental overreach.
Heather Wargo has been published by The Western Journal, Lifesite News, The Ascent, P.S. I love You, Publishous, Uncalendared, The Writer’s Cooperative and Writer’s Guild.
Just about every patient I advocate for in the incurable painful disease patient community has asked me one question I was never able to answer.
Because it also danced in MY mind.
Why are they doing this to us? Why are they taking medicine away from people like us?
The data wasn’t supporting what all the pundits said on the news.
The media was desperately pushing a narrative.
But why?
The Plan
The United States Government, through the CDC, has implemented a massive society based clinical trial/population based study, largely executed through the creation of the Centers for Disease Control’s 2016 Guidelines for Opioid Prescribing for Treatment of Chronic Non Cancer Pain. This is real, it is true.
Not one Congressional or Senatorial office denied this research when confronted with the evidence.
Senator Gillibrand’s office pathetically tried to gaslight the whistleblower. While responding, the whistleblower says, “It is clear to me this is about liability, not the public’s health and livelihood.” Her staffer sneered, “Of course, it’s about liability!”
The evil plot originated in Washington State in the late 2000’s, when a group of powerful men and women met to discuss how fed up they were with paying out worker’s comp, along with their unshakeable belief that people who use opioid medication to control pain are “just sitting at home getting high” instead of being a productive worker.
Most of them firmly believe opioid therapy users are just junkies.
Participants included future PROP (Physicians for Responsible Opioid Prescribing) members who had been studying workers comp since the 90’s, along with stakeholders in data surveillance, universities, social marketing, media, and of course, the main driver — insurers. They began pushing and publishing study after study to craft the narrative they wanted.
March 23, 2010, the ACA was rammed into law, unread, granting HHS, CDC, and the Office of the Surgeon General powers previously unheard of.
2010/2011 Dozens of innocently named agencies were formed, all with one purpose — getting patients completely off their opioid therapy — we will see these all listed in Part II and what they “do”. Section 4305 of the ACA was about pain management and void of most targeted particulars.
2010 — Present Surveillence of citizens through Brandeis’ PDMPs begins through widespread state system use. No consent obtained, of course. Surveys and studies are pushed through EHRs, every nook and cranny of medicine, all “voluntary” yet not, because patients must answer all questions to receive care. Ongoing to date. Taxpayer funded.
2012- The Institute of Medicine (those sneak thieves who renamed themselves the “Health and Medicine Division” the day the CDC Guidelines were issued) quietly published an e-book titled “Living Well with Chronic Illness- A Call for Public Health Action” — basically the groundwork for the CDC guidelines, it calls for a study to be performed of every single population in America. (except WHITE MALES). It sets the stage for pain to be dismissed and for people to be gaslighted if they say they have pain.
2013- ongoing The Boomers are becoming old, sick, disabled, and in pain. Many of whom were injured in war or gov. jobs. The largest working generation was going to be cashing in their legit earned Social Security. This is not wanted or desired. Instead, our eugenicists wanted to make it hell on earth for those Boomers, so their money stayed in the gov. See part II.
2014 Appriss uses a study done in Ohio to unleash Narxcare, a “ranking system” that uses proprietary algorithms to practice medicine, telling a doctor whether or not a patient should or should not receive medication based on a score. Even recommending rehab. Patients are never told about this system or scoring, in fact patients are told they are not allowed to know.
2016. 03.16 — Six Building Blocks Grant Funds — THE COUP de GRACE — DAY the CDC Guidelines were Issued, March 16, 2016, HHS released funding to the states. Monetary grants were given, millions of dollars. States received these from HHS to begin implementing the “6 Building Blocks” Plan through the Office of Surgeon General National Prevention Strategy’s National Prevention Council (one of those lovely ACA groups). THE DAY OF THE GUIDELINES — — The exact grants & grant numbers will be shown in Part II. (side note — remember this when FDA attempts to dazzle with their breathless release of “We pledge $20 million to fight illicit fentanyl!”) Wow, how generous to pledge pocket change to fight an actual proven killer of American teenagers/young adults. It’s like they don’t even care, or something.
2010/2012/2015/2018- Agency for Healthcare Research and Quality (AHRQ)- National Guideline Clearinghouse is officially defunded on July 16, 2018 after several attempts, 2010, 2012, 2015, 2016… This agency was the overseer to “produce evidence to make health care safer, higher quality, more accessible, equitable, and affordable, and to work within the U.S. Department of Health and Human Services and with other partners to make sure that the evidence is understood and used” as per their original mission statement- lost to the ether. Of course this place has to go. It has been replaced with a newer vision — The 6 Building Blocks!! How circular!
Ongoing — Pain Advocacy Groups/ Social Media infiltration by Government Agents. This will be discussed to show the real patients they have been duped by faux groups and people into believing they are “being represented” by those who want to “help” painful disease patients, when in reality they are merely being studied by these people and lied to by covert, government operated people, physicians, and orgs.
MORE… so much more.
Is this incredible, unbelievable? Yes.
Is it true? Yes. All of it.
Just consider one thing. Why would the CDC change any part of their guidelines after two years of nonstop begging by every single advocate group, patient and pain affiliate in America?
It is NOT because of some letter they received in November. Please. More on that con in Part II also.
CIAAG founder Lauren Deluca and board member Shasta Rayne Harner took these findings of fact they discovered independently through their very own research to Washington D.C. on Monday, April 8, 2019, to let Congress know the gig was up.
They spent three full days in meetings with Congress, Reps., & Senators, 4/8/2019–4/10/2019 while others played pretend.
Some time ago, I was informed of their findings, asked to assist with research moving forward, and asked to write about this horrific con job perpetrated upon the American people.
I am not a CIAAG member. I share a mutual relationship of shared respect and interests with its founder and board. No one is being paid — not here.
This has been an ongoing investigation by CIAAG. No one else.
What — are these others going to investigate… themselves?
In part II, you will see a plethora of findings of fact.
I recently saw an old man and his grandson getting arrested outside the local CVS while I was filling one of my Rx. From what I overheard the grandfather could not afford his Rx so his grandson paid for it with his credit card. The pharmacist filled their RX of course.then called the police because the grandson had a different last name as his. The pharmacist could have warned them or not filled it but no… He filled it anyway… They surrounded them in the parking lot.
They were in no hurry to leave, they had no idea they had done anything wrong… The police had them both spread across the hood of the cop car pouring out the bottle of pills across the hood on display like it was crack or something… The wind was blowing and several times before they had them in the squad cars had to stop to pick up the old man’s pills off of the road…. God I wish my phone had not been almost dead I’d have recorded the whole thing… I have no idea if they were or were not guilty of any actual crime but from what I overheard I pray that they are found not guilty and Sue for wrongful prosecution. But I’m sure in our quickly declining morally bankrupt society they probably won’t have a leg to stand on…. God help us all….
I had to give this some thought… Other than being totally irrational.. did the Pharmacist JUMP TO THE CONCLUSION that the Senior Citizen was selling his medication to the younger kid ?
Of course now, the pt’s medication is contaminated and or destroyed regardless of the outcome. And the Grandson will have – most likely – have to pay for the medication put on his charge card.
Should/could the Pharmacist be charged with making a FALSE POLICE REPORT ?
Is this Pharmacist so anxious to “bust someone” trying to illegally obtain a controlled substances that his “common sense” has been overtaken by his paranoia ?
Four doctors in Carmel, IN, a suburb of Indianapolis, have sued the city and government officials responsible for the illegal attack on their clinic, Drug Opiate & Recovery Network (DORN), an addiction center prescribing Suboxone, in July, 2014. The lawsuit asks for compensatory and punitive damages and requests a jury trial. Drs. Larry Ley, founder, George Agapios, Ronald Vierk, and Luella Bangura were all arrested and charged, in spite of years of continuous communication with DEA officials. This shows the evil in the DEA.
“They destroyed the lives of 12 people that were actively trying to fight this disease, and they threw all the patients who were actively fighting addiction to the curb,” said Dr. Ley. In spite of the charges being dropped against them, or the acquittal of Dr. Ley, shedding the stigma of the raid has proved difficult for the clinic’s doctors and staff since the arrests, which is why they decided to take legal action. The employees have been unable to find other work, even though their records have been expunged.
The attorneys for the city and some of the officials have declared immunity in the lawsuit. That is the protective umbrella by which these unscrupulous DOJ officials are carrying out illegal attacks against legitimate practitioners across the country, and something we, the citizens, must remove. If a government official knowingly attacks an innocent citizen for illegal purposes, that official should be held accountable. If not, this country is moving into a police state. The plaintiffs’ claims of false imprisonment and arrest are also possibly barred due to a probable cause being filed in the case, even though that probable cause was created through perjury. Also, to show how the DOJ colludes in their illegal attacks on doctors, Assistant U.S. Attorney Josh Minkler who was first offended by the behavior of DEA agent Gary Whisenand pushing the case against Dr. Ley, is now representing Whisenand in the civil suit.
The new complaint of false arrest and violating their right to due process is against DEA agent Whisenand, the city of Carmel and Major Aaron Dietz of the Hamilton/Boone County Drug Task Force. But Dietz’s attorneys claim he was acting in good faith and is therefore immune from civil action under law. Good faith—Bull shit!! The target was picked, the case was created.
In the government’s standard propagandizing media collusion when doctors are attacked, Dietz was quoted as saying
“We make no distinction between Dr. Ley and any other drug dealer,” calling the clinic a “pill mill” and Dr. Ley “the Pablo Escobar of Suboxone.” “This type of ruse of a clinic perpetuates the problem. Those people are still addicted to the drug and this is what’s happening. This is not fixing the problem,” “Opiate drugs and prescription medication is a gateway to heroin. That’s why we have heroin is because people get addicted to the opiate drug prescription medication and then go to a cheaper, readily available heroin.”
Now all of those statements are lies stated in public to defame a proper, law-abiding citizen. Shouldn’t that perpetrator of illegal activity (Dietz) have to pay for his crimes?
Dietz and Whisenand worked for months to create a case against the doctors. This is an example of tax dollars being wasted. They spent nine months watching hundreds of patients comes and go from the clinics, compiling more than 26,000 hours of video surveillance in the process. But they were unable to identify a single individual who was paying for a drug they didn’t legitimately need. So they invented some by sending undercover officers to lie about being dependent on opiates. So probable cause was a creation of the government.
Then, despite being told twice by the U.S. attorney’s office that they didn’t have a case against Ley, they arrested Ley and 11 of his employees for “providing Suboxone prescriptions to the undercover officers who had no legitimate medical need for them.”
This is a standard practice in all attacks on doctors, and primarily what they are being convicted of: “illegitimate medical practice” because the DEA agents lie to get drugs prescribed that they don’t really need. Who’s committing the crime here? But as the suspected “ringleader” of the operation Ley was booked on $1 million bond, his assets seized, and he spent a month in jail.
One by one the cases against Ley’s 11 co-defendants fell apart, as prosecutors failed to provide enough evidence that a crime had been committed. Dr. Ley was the only DORN defendant to go to trial. The charges against him applied to just 22 prescriptions for Suboxone—all written to police officers pretending to legitimately need them. That fact was not lost on Hamilton County Judge Steven R. Nation, presiding over Ley’s trial.
“I struggled with this case the minute I started to watch the surveillance videos [of the undercover agents],” Nation said, prior to announcing Ley’s acquittal. “I’ve got conditions that people were asking to be treated for [and] the drug that was issued was appropriate for what they were being asked to be treated for.”
Why aren’t more judges seeing this fact? Maybe because they ride the gravy train of convictions too? Judges are not unbiased in these cases where money is funneled into the Department of Justice and their own courts. Ethics and morals are found less and less in the legal profession. But at least in this case under this judge, Ley was cleared of all charges after an eight-day bench trial and all other charges against him in other counties where he ran clinics were dropped.
Jim Crum, Dr. Ley’s defense attorney stated what every defense across the country should be stating:
“Our position has been, and the judge agreed, that the judges point that if there was a violation of anything here it’s a licensing issue.” Is the doctor following the rules exactly? “Even if he wasn’t that doesn’t rise to the level of a criminal offense. There was no intent to deal, everything was in the confines of the normal practice of medicine.”
James Brainard, Mayor of Carmel
Dr. Ley was acquitted in August 2016, two years after the raid. Similar clinics across the country are being attacked and the doctors incarcerated. But here, the reason is obvious—a politically motivated effort to help developers in Carmel, directed by Mayor James Brainard. I won’t go into the possible collusion between Mayor Brainard, the Carmel Redevelopment Commission, and Pedcor here. But a detailed review of public records showed that the city had its eye on the property before Dr. Ley became a subject of a criminal investigation. In 2016, just months before the start of Ley’s trial, the city of Carmel revealed a takeover of the property across the street and construct a new mixed-use development called the “PNC Block Redevelopment” involving condominiums, commercial office space, underground parking, and an outdoor beer garden. If the goal was to force Ley out of Carmel, a conviction wasn’t necessary. DORN’s main office in Carmel never reopened, and Ley sold it for a loss to a real-estate investor.
So what is the result of attacks on legitimate clinics like this on the occurrence of addiction? Use Indiana as an example. Thanks in part to the policies of former Indiana Governor Mike Pence, treatment options in Indiana were limited even before Dr. Ley’s arrest. The state ranked 47th out of 50 states for availability of drug and alcohol treatment and Suboxone treatment was among the worst in the nation. Hamilton County ranked ninth out of 92 counties for heroin overdoses. In Indianapolis drug overdose fatalities increased seven-fold since 2000. Hamilton County alone has seen a 45 percent increase in heroin-related deaths. In 2015 more than 300 non-fatal overdoses were recorded in the four counties where Ley practiced. Two years after the closure of the DORN clinic, fatal overdoses in Indiana have risen by double digits, with only three providers certified to prescribe Suboxone in the entire city of Carmel.
This is a excellent example of the mindset of our society.. ONCE CHARGED – ALWAYS GUILTY .. REGARDLESS OF BEING INNOCENT IN THE END ! Did the City of Carmel and the bureaucrats of that city wanted to have the property that Dr Ley owned for development so that the city could generate more property tax revenue and they would not have to go thru imminent domain and have to pay “fair value” for the property ?
It is claimed that “JUSTICE is BLIND” … but apparently for those within our justice system appear to be driven by GREED and monetary gains the judicial system can reap by “going after” certain segments of the population that has assets/resources that they can fabricate a case against and according to this article many judges and prosecuting attorneys are more than willing to be willing participants in this ruse.
At one time, Indiana was ranked NUMBER ONE in pharmacy robberies and NUMBER ONE in meth lab busts and then in 2015 had 200 people show up being HIV positive along with Hep B & C.. in small (pop 25,000) Scott County in south central Indiana.. which DNA testing showed that abt 85% was from a single source. Meaning that most of those people where involved with sharing needles.
Then Gov Pence – now VP Pence – his response to that outbreak was quite interesting .. basically he was CLUELESS about how to proceed at first. It was like the fire dept showing up with a 5 lb fire extinguisher when your house is on fire.
CVS Pharmacy just announced their pharmacist working hour cuts. “Verification sharing”, a technological workload share computer program, is now leading to sweeping hour cuts and overlap diminishes across our district and our neighboring district, and I’m certain the whole company chain. In my store, hours has been cut 8 full RPh hours, many others are seeing more hours cut. For a company that says they value patient safety, they are not giving us the tools we need to keep people safe. By cutting pharmacist hours, this will increase wait times and our current inabilities to get medications into the hands of our patients that need them. A deliberate move to continue lining the pockets of the top executives.