


Filed under: General Problems | 5 Comments »










Email steve@steveariens.com 502-938-2414




Pay Attention



Filed under: General Problems | 5 Comments »
The Drug Enforcement Administration has proved itself incompetent for decades.
www.nytimes.com/2018/09/17/opinion/drugs-dea-defund-heroin.html
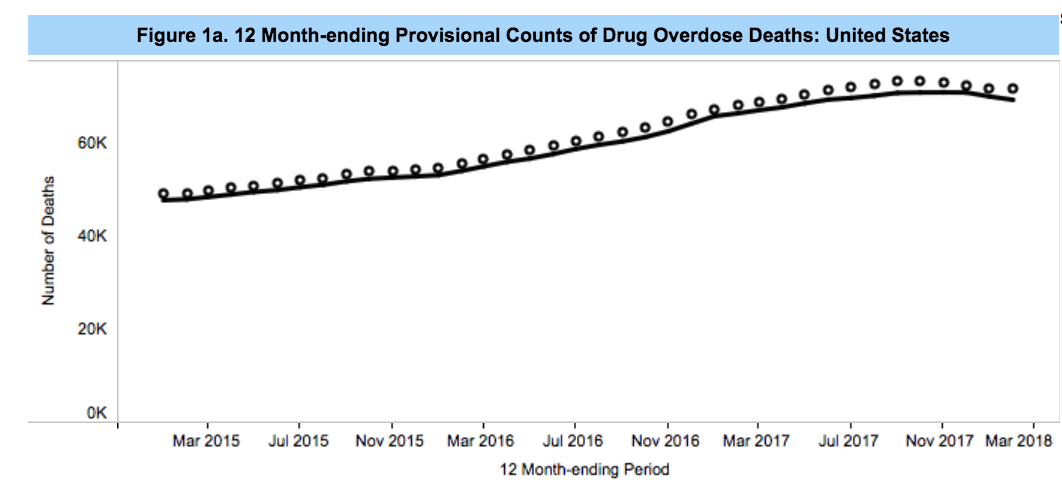
Every day, nearly 200 people across the country die from drug overdoses. Opioids have been the primary driver of this calamity: first as prescription painkillers, then heroin and, more recently, illicitly manufactured fentanyl. The death toll has risen steadily over the past two decades.
The Drug Enforcement Administration, the agency that most directly oversees access to opioids, deserves much of the blame for these deaths. Because of its incompetence, the opioid crisis has gone from bad to worse. The solution: overhauling the agency, or even getting rid of it entirely.
The problem begins with poor design. A brainchild of Richard Nixon’s “war on drugs,” the agency sought to cut off supplies of drugs on the black market, here and abroad. But in passing the Controlled Substances Act of 1970, Congress also gave the agency broad authority over how prescription opioids and other controlled substances were classified, produced and distributed. The agency was supposed to curb problematic drug use, but failed to do so because its tactics were never informed by public health or addiction science.
Despite the investment of hundreds of billions of taxpayer dollars and the earnest efforts of thousands of employees, the D.E.A.’s track record is abysmal. The agency has been unable to balance legitimate access to and control of prescription drugs. The widespread over-reliance on opioids, along with benzodiazepines, amphetamines and other scheduled medications, has created a booming black market.
The agency’s enforcement strategies, and the support it has lent to local and state police departments, have also fueled abusive police tactics including dangerous no-knock-raids and ethnic profiling of drivers. It has eroded civil liberties through the expansion of warrantless surveillance, and overseen arbitrary seizures of billions of dollars of private property without any clear connection to drug-related crimes. These actions have disproportionately targeted people of color, contributing to disparities in mass incarceration, confiscated property, and collective trauma.
The United States was ill equipped to navigate the worst drug crisis in its history with the D.E.A. at the vanguard. Starting in the late 1990s the manufacturing, distribution and prescribing of opioids began to increase rapidly. Overdose deaths soared since so many people were prescribed opioids and many mixed them with alcohol and other sedative drugs. The D.E.A. could have marshaled a calibrated response, expanding evidence-based treatment and reducing the prescription of especially risky drug combinations.
Instead, the agency pushed for surveillance of prescription records and electronic communication, doubled down on prosecuting prescribers and helped to tighten the screws on patients seeking pain relief. Meanwhile, lifesaving opioid treatments that the D.E.A. closely regulates, like methadone, have remained extremely difficult to obtain. Indeed, these problems were much broader than the alleged industry machinations to muzzle the agency.
A decade into the crisis, more and more prescription drug users turned to the black market. Even though the D.E.A. had tried to “eradicate” illicit drugs for nearly 50 years, users could easily buy stolen and counterfeit pills, along with a cheaper option, heroin. Soon, some began injecting. Outbreaks of H.I.V. and hepatitis C followed. Meanwhile, people who sought evidence-based treatment were rarely able to access it because of the agency’s evolving regulatory and enforcement strategies, like blocking the expansion of mobile methadone clinics and shutting down addiction treatment providers without arranging alternatives for affected patients.
As the engine of overdose deaths shifted from prescription drugs to heroin, the D.E.A. turned to its supply-reduction playbook. This resulted in a major uptick in heroin seizures and high-profile prosecutions, which encouraged traffickers to create more compact, potent drugs. In a single year, from 2014 to 2015, deaths involving the synthetic opioid fentanyl and its analogues almost doubled, setting the stage for its current role as the principal driver of overdose fatalities. And since 2015, the agency has not had an appointed administrator.
We urgently need to rethink how our nation regulates drugs. What should our goals be? How can we design institutions and performance metrics to achieve them?
The answers lie at the local and state levels. In Rhode Island, opioid overdoses are declining because people behind bars have access to effective treatment. Massachusetts has deployed drop-in centers offering treatment, naloxone and other services. San Francisco and Seattle are planning to open safe consumption spaces which show tremendous promise as a tool to reduce overdose deaths and other drug-related harm. But the D.E.A. and its institutional parent, the Justice Department, stand in the way of some of these experiments.
We ought to reinvent the Drug Enforcement Administration. Considering its lack of public health and health care orientation, the agency’s regulatory authority over the pharmaceutical supply could be transferred to a strengthened and independent Food and Drug Administration, while the regulation of medical and pharmacy practice can be ceded to the states. Parts of the D.E.A.’s law enforcement mandate should be transferred to the F.B.I., delegated back to the local or state, or eliminated. A significant portion of the D.E.A.’s budget should be reinvested in lifesaving measures like access to high-quality treatment.
The Drug Enforcement Administration has had over 40 years to win the war on drugs. Instead its tactics have fueled the opioid crisis. To finally make a dent in this national emergency, we need to rethink the agency from the bottom up.
Leo Beletsky, an associate professor of law and health sciences at Northeastern University, is the faculty director of the Health in Justice Action Lab, where Jeremiah Goulka is a senior fellow.
Filed under: General Problems | 1 Comment »
WASHINGTON — The Senate on Monday overwhelming approved a sweeping legislative package of bills aimed at combating the nation’s deadly opioid epidemic.
The bipartisan measure passed 99-1. Sen. Mike Lee, R-Utah, was the only senator to vote against it.
Similar to the House package passed in June, the Senate’s Opioid Crisis Response Act of 2018 (OCRA) directs funding to federal agencies to establish or expand programs dealing with prevention, treatment and recovery.
Highlights from the 70 bills in the package include funding that requires the Food and Drug Administration to dole out prescription opioid pills in smaller quantities and money that offers an incentive to the National Institutes of Health to prioritize the development of non-addictive painkillers, two solutions medical experts believe could help decrease opioid addiction in the long run.
The package also includes Ohio Republican Sen. Rob Portman’s Synthetics Trafficking and Overdose Prevention Act “STOP” Act, a bill endorsed by President Donald Trump because it establishes parameters to crack down on shipments of fentanyl, a synthetic opioid, from entering the U.S.
Currently, the U.S. Postal Service is the only transportation carrier that does not collect electronic information on overseas cargo, which makes it harder for Customs and Border Protection agents to screen packages for drugs.
The Senate package comes months after the House passed their 58-bill opioid package, a response to the pressure lawmakers have felt to find solutions for the deadly crisis that has affected every state in the country.
Overdose deaths killed an estimated 72,000 Americans in 2017, according to the Centers for Disease Control and Prevention. In comparison, over 40,000 Americans died that same year in car accidents, while 12,000 died from gun violence.
The Senate vote on Monday also offers a success for vulnerable Democrats and Republicans to point to during the final weeks leading up to November’s midterm election. Some of these lawmakers have seen ads in their states pressuring them to support opioid legislation.
In an effort to secure a massive bipartisan legislative win before year’s end, the chairman of the Senate Committee on Health, Education, Labor and Pensions, Lamar Alexander, R-Tenn., spent a majority of the summer leading an effort to hammer together dozens of bills passed by five Senate committees this year.
Three sources familiar with the process tell NBC News the Senate and House have already started to iron out minor differences in their legislative packages, including parameters for opioid addicts to access Medicaid-backed mental health facilities. Currently, the Senate version also reauthorizes $500 million per year in opioid grant extensions for the next three years, includes provisions for doctors to understand how to treat young addicts. It also reauthorizes the White House’s ability to oversee narcotic-related issues among federal agencies.
Once a compromised bill is worked out, each chamber will have to pass the bill before sending the final measure to the president for his signature.
 Something that all the members – except one (Sen. Mike Lee, R-Utah) – can agree upon… talk about your bipartisan bill… The House passed this bill in June and now a vote of 99-1 in the Senate it is going to Pres Trump to be signed into law. It only took 70 DIFFERENT BILLS to address the singular opiate crisis. Another complex solution to a potentially very simple problem … provided by our Congress..
Something that all the members – except one (Sen. Mike Lee, R-Utah) – can agree upon… talk about your bipartisan bill… The House passed this bill in June and now a vote of 99-1 in the Senate it is going to Pres Trump to be signed into law. It only took 70 DIFFERENT BILLS to address the singular opiate crisis. Another complex solution to a potentially very simple problem … provided by our Congress..
In Nov, 435 members of Congress and 33 Senators are up for election in Nov … that means that 87% of Congress is up to the voters if they go back to be a member of Congress starting in Jan 2019.
This Congress is not going to help the chronic pain community… does it really make any difference if they were all tossed out of office and a whole bunch of novices takes over Congress in Jan 2019 ?
They have discounted your pain… they have encouraged your TORTURE… they have ignored the TRUTH and FACTS… they have DISCARDED your comments, Dozens or HUNDREDS of petitions have been discarded… Your reality is not their reality… Do they deserve YOUR VOTE ?

Filed under: General Problems | 4 Comments »
Roseanne Barr revealed how her character will get killed off on the upcoming spinoff of “Roseanne” after she was fired from the ABC series in May for writing a racist tweet.
Barr told Brandon Straka on his YouTube show “Walk Away,” that the
“Oh ya, they killed her,” she said. “They have her die of an opioid overdose.”
A rep for “The Conners” did not immediately return Fox News’ request for comment.
Barr made it clear she was not happy with her character’s fate saying it was disrespectful to fans “who loved that family” on the original series.
“There’s nothing I can do about it,” Barr admitted. “It’s done. It’s over.”
Barr’s former co-star John Goodman revealed previously that her character would die in the spin-off but did not say how. ABC has yet to comment on how they will handle Barr’s character’s death.
Barr made headlines after she tweeted in May that former President Barack Obama’s aide, Valerie Jarrett, who is African-American and was born in Iran, was as though the “Muslim brotherhood & planet of the apes had a baby.” ABC canceled the popular reboot of “Roseanne” shortly after the tweets.
In case anyone is interested…. ABC is owned by The Walt Disney Company and here are some of the other major companies that The Walt Disney Company owns …
https://www.investopedia.com/articles/markets/102915/top-5-companies-owned-disney.asp
Here are just a few of the mouse house’s biggest companies:
Disney/ABC Television Group operates Disney’s broadcast television, cable television and radio businesses. Its broadcast TV businesses include ABC Studios, ABC News and the ABC Television Network, which combine to deliver programming to more than 200 local TV affiliates across the country. Disney/ABC Television Group also operates eight local television stations in some of the country’s biggest media markets. On the cable side, Disney/ABC Television Group operates the ABC Family channel and Disney Channels Worldwide, a unit that includes more than 100 Disney-branded cable networks reaching 164 countries and territories around the world.
Disney/ABC Television Group also has equity stakes in three independently operated media businesses: A&E Television Networks, Hulu, and Fusion Media Network. A&E Television Networks is an equally held joint venture with the Hearst Corporation. It operates a variety of cable channels, including A&E, History and Lifetime. Disney/ABC Television Group has a 30% stake in Hulu, an online streaming video service featuring ABC Studios content. Disney would have a controlling stake in Hulu if the Fox deal goes through. Fusion is a multi-platform media company targeted at Hispanic Americans. It is an equally held joint venture with Univision Communications, an American media and broadcast company.
ESPN is a sports media and entertainment company with eight cable networks in the U.S. and another 16 TV networks abroad. Disney holds a controlling 80% stake in ESPN, while Hearst Corporation owns 20%. In addition to its TV properties, ESPN operates other related media businesses, including ESPN.com, ESPN Radio, and WatchESPN. ESPN also holds a 30% stake in CTV Specialty Television, a multichannel Canadian sports broadcaster.
Walt Disney Parks & Resorts U.S., Inc. operates Disneyland in California, Walt Disney World Resort in Florida, and Aulani, a spa and resort in Hawaii. These operations include numerous company-owned hotels, retail and entertainment complexes, conference centers, and indoor and outdoor recreation facilities. Walt Disney Parks & Resorts also operates Disney theme parks overseas through a handful of international subsidiaries.
Disney Parks & Resorts’ French subsidiary, Euro Disney S.A.S., owns 51% of Disneyland Paris. In China, Shanghai International Theme Park Co. controls 43% of Shanghai Disneyland Resort, Hong Kong Disneyland Management controls 47% of Hong Kong Disneyland Resort. While Walt Disney Parks & Resorts does not have an ownership stake in Japan’s Tokyo Disney Resort, it does earn licensing royalties from the Japanese operating company, Oriental Land Co.
In early February of 2018, Disney announced it would be increasing the ticket prices for its American-based theme parks by around 9%, with a regular adult one day pass at the Magic Kingdom in Orlando costing $129, instead of its former price of $124.
Lucasfilm is a film production company best known for producing the Star Wars and Indiana Jones series, two of the biggest-grossing film franchises in history. Disney acquired Lucasfilm in 2012 for $4.06 billion. Its subsidiary media and production businesses include Industrial Light and Magic, Skywalker Sound, and Lucas Licensing. Under Disney’s watchful eye, the company has started a new line of Star Wars films, and has plans to create a fifth Indiana Jones film starring Harrison Ford in 2019. According to the Hollywood Reporter, the company made back its purchase of Lucasfilm in late 2017 when The Last Jedi brought the total gross of these new Star Wars movies to $4.08 billion, on par with the initial buy.
Marvel Entertainment is a media and entertainment company with operations in publishing, television, and film. Marvel is best known for its catalog of fictional characters, including Spider-Man, Captain America, and the X-Men. Disney acquired Marvel and the rights to its more than 5,000 characters in 2009 for $4 billion. Marvel’s blockbuster superhero films have gone on to be huge earners for Disney, giving the company high spots on the top 10 highest grossing movies of the year for several years now. Marvel Entertainment’s subsidiaries include Marvel Studios, Marvel Animation and Marvel Comics.
Filed under: General Problems | 2 Comments »
 Coca-Cola ‘Closely Watching’ Use of Cannabis in Wellness Drinks
Coca-Cola ‘Closely Watching’ Use of Cannabis in Wellness DrinksWhile Coke may be looking into the potential of marijuana-infused health beverages for pain relief, the company has no interest in helping consumers get high.
The Coca-Cola Company released a statement on Monday following reports indicating that the beverage behemoth was looking into possibly infusing drinks with cannabidiol, a non-psychoactive component in cannabis commonly known as CBD.
“We have no interest in marijuana or cannabis. Along with many others in the beverage industry, we are closely watching the growth of non-psychoactive CBD as an ingredient in functional wellness beverages around the world,” the company said.
What gets people high from marijuana is not CBD but tetrahydrocannabinol, the potent psychoactive chemical compound commonly known as THC.
BNN Bloomberg first reported that Coca-Cola and cannabis producer Aurora Cannabis Inc. were engaged in talks to possibly develop health-focused beverages geared toward pain relief. Neither company has confirmed any plans.
“The space is evolving quickly. No decisions have been made at this time,” Coca-Cola’s statement said.
The report comes as more U.S. states move to legalize marijuana for recreational use and as Canada, where Aurora is based, prepares to fully legalize the recreational use of cannabis next month, CNBC reported.
CBD advocates say the chemical compound can provide multiple health benefits, including pain management and treatment for seizures and neurological disorders.
Despite the growing number of states legalizing marijuana for medical and recreational use, the federal legal status of CBD in the U.S. is still somewhat cloudy. Marijuana is currently a Schedule I drug under U.S. Drug Enforcement Administration guidelines, which means the agency considers it to have no accepted medical use and a high potential for abuse.
But the DEA this year clarified that CBD did not fall under the definition of marijuana per the Controlled Substances Act, because the method to extract the compound would leave behind only trace amounts of illicit cannabinoids.
And in late June, the U.S. Food and Drug Administration for the first time approved a prescription drug made from CBD to treat two rare forms of epilepsy.
Filed under: General Problems | 1 Comment »
https://www.healthaffairs.org/do/10.1377/hblog20180913.889578/full/
Recently, CVS Health announced a new formulary management option: allowing self-insured employers to remove from their formularies medicines launched at a price greater than $100,000 per quality-adjusted life-year (QALY). The New York State Drug Utilization Review Board has also recently used a cost-effectiveness threshold to justify its mandate for the Medicaid program to receive a steep discount on the price of a cystic fibrosis treatment. If the discount is not obtained, access to the drug will likely be limited. Both CVS and the New York State Board based these decisions on cost-effectiveness estimates from the Institute for Clinical and Economic Review (ICER). Although there is strong support for the movement toward value-based care and prices, the CVS option and New York’s decision for its Medicaid program are too much too soon and could hamper patients’ access to needed medicines, for the reasons described in this post.
First, cost-effectiveness is an element of value, but it is not synonymous with it. Multiple groups in the US, such as the ICER, the American Society of Clinical Oncology, the National Comprehensive Cancer Network, the Innovation and Value Initiative, and Faster Cures, among others, have proposed value assessment frameworks. None uses cost-effectiveness as the sole measure of value. To fully assess the value of a treatment, stakeholders must account for other considerations important to patients. Examples of these other considerations include: a new therapy’s ability to treat a previously inadequately treated illness; its ability to broaden therapeutic options for diseases with great variability in treatment response; the possibility of cure and the importance of hope related to it; the ease of a regimen when alternative therapies are complex, cumbersome, and time consuming; or, its novel mechanism of action that could lead to markedly improved derivative treatments. Although the National Health Service (NHS) in the United Kingdom bases many of its coverage decisions on the National Institute for Health and Care Excellence’s cost-effectiveness assessments, even it incorporates other considerations, and the strict NHS approach has not garnered real support from stakeholders in the US.
Second, the CVS program uses a threshold of $100,000 per QALY and likely will use a health system perspective that does not incorporate the economic value of improvements in productivity or reductions in caregiver burden. The scholarly, Second Panel on Cost-Effectiveness in Health and Medicine, which provided the latest broad overview of how these assessments should be performed, has emphasized the importance of considering not just the health system perspective but also the broader societal one, which incorporates these indirect benefits. Moreover, the CVS plan has a single economic threshold ($100,000). In contrast, ICER’s value framework – which has the greatest focus on cost-effectiveness among all the frameworks — has a variable threshold (sometimes $100,000, other times $150,000) based upon the other considerations beyond the cost-effectiveness listed above. Evaluating all therapies for all diseases under all circumstances with a single threshold is an inappropriately blunt approach. CVS mentions that its approach will not apply to medicines deemed “breakthrough therapies” by the Food and Drug Administration (FDA). If CVS believes that the breakthrough designation connotes important non-economic considerations, then why just consider the FDA designation and not the factors above?
Third, CVS proposes a dichotomous view of a treatment’s value. If the cost-effectiveness assessment is below $100,000 per QALY, then the formulary would include the medicine, and if the assessment exceeds the threshold, it would not. What about medicines with a cost-effectiveness of $105,000 per QALY? Premera Blue Cross uses cost-effectiveness in constructing its formularies but has a more nuanced approach. The company ties formulary tiers, and thus copayments, to cost-effectiveness. Rather than denying patient access, Premera makes a broader set of medicines available but adjusts how much the patient pays for medicines it deems to have lower economic value.
Fourth, by making a dichotomous formulary access decision based upon a single cost-effectiveness number, CVS presupposes that all patients respond in the same fashion to a therapy. There is substantial literature demonstrating heterogeneity of treatment effect, which means that for the same treatment, some patients benefit far more than the average. The CVS approach ignores this important clinical component.
Finally, in allowing its clients to use ICER’s cost-effectiveness assessment as the sole source of data to support formulary exclusion, CVS assumes that the field of value frameworks is fully mature, has addressed the many limitations of the QALY, and is ready for prime time, which it is not. Last year in a Health Affairs blog, we identified six key considerations for the improvement of value frameworks, as follows:
Prices should reflect value, and concerns about health care spending should move us toward incentivizing high-value interventions and dis-incentivizing low-value care. However, the announcement from CVS, perhaps well intentioned, is too much too soon.
Filed under: General Problems | Leave a Comment »
https://www.kansascity.com/news/politics-government/article199431699.html
U.S. Sen. Claire McCaskill thinks her mother was addicted to opioids before she died.
McCaskill, a Missouri Democrat, hosted a health care roundtable Friday afternoon at St. Luke’s Hospital.
The roundtable with Kansas City physicians and other medical professionals covered topics including the cost of emergency room care, the impact of Missouri’s decision to not expand Medicaid and problems in the state’s mental health system.
McCaskill also devoted several minutes to the highly personal topic of opioid addiction and the intensive outpatient treatment programs that exist in her neighborhood.
“There’s no question my mom was addicted to opioids near the end of her life,” said McCaskill, whose mother, Betty Anne McCaskill, died in 2012 at age 84.
She recalled how her mother often told her doctors that her pain was at a 10 on 1-to-10 scale to get the strongest dose of medication during her final years.
Marc Larsen, the chair of emergency medicine at St. Luke’s, told McCaskill the medical community “created this epidemic by saying we have to treat the pain.”
McCaskill, who has led an investigation into opioid manufacturers, floated the idea of broadening her investigative efforts into the rest of the pharmaceutical industry. She repeatedly expressed her concern about the links between drug companies and research organizations that tout the benefits of medication.
Another area of focus during the discussion was the state of mental health care in Missouri.
McCaskill was shocked to learn that the largest mental health care provider in the state is the Department of Corrections. She was also surprised to learn that Missouri incarcerates women at a higher rate than any other state.
“Are women meaner in Missouri?” she quipped.
After the meeting, she blamed both of these statistics on the state’s “failure to have wrap-around health services, mental health services, behavioral health services for many of the underinsured and uninsured in our state.”
Another person with a LAW DEGREE making medical opinions and decisions. McCaskill is up for RE-ELECTION in November.. She has been in the Senate for 18 yrs… Is it time for some TERM LIMITS being applied to her ?Filed under: General Problems | 2 Comments »

ATTN USA! “Health” Insurance companies are limited to 15% profit margin, BUT their PBM’s can take 70% profit! Insurance company/PBM mergers are taking place right under our noses! Absolute THEFT from the American people under cover of “universal coverage!”

Filed under: General Problems | Leave a Comment »
https://www.buzzfeednews.com/article/danvergano/heroin-use-drops
Amid staggering numbers of fatal US drug overdoses, fewer people started using heroin in 2017 — the numbers dropping by more than half — a new federal survey suggests.
The Substance Abuse and Mental Health Services Administration (SAMSHA) on Friday released its long-running National Survey on Drug Use and Health (NSDUH), which surveys illicit drug use nationwide.
The yearly survey’s results are the vital signs of a nationwide drug overdose epidemic that killed around 70,000 people last year and was declared a national public health emergency by President Trump.
About 44,000 of those deaths came from heroin and related synthetic opioids such as fentanyl, which is many times more potent with notorious overdose risks. According to the group, which surveyed more than 60,000 people, there are about 500,000 people in the US who are users of heroin.
It’s possible that these high fatal overdose numbers are starting to sink in with illicit drug users. Last year, the number of new heroin users in the US dropped by 53% to 81,000 people, according to the survey’s findings. That’s down from 170,00 in 2016.
The survey also found “a significant increase” in people receiving specialty treatment for illicit drug use disorders. “This was particularly evident for those with heroin use disorder and opioid use disorders,” according to a SAMSHA summary of the findings.
“Great news,” medical epidemiologist Daniel Ciccarone of the University of California, San Francisco, told BuzzFeed News.
Drug users aren’t happy with the increase in fentanyl — a highly potent synthetic opioid that’s often mixed into heroin and is the cause of many overdoses — showing up in their drug supply, which could lead to fewer people starting on heroin in the first place, he added.
While deadly drugs like fentanyl can discourage new drug users, these opioid drugs are also responsible for strong physical dependencies in existing users, making it harder to kick the habit. This could extend the duration of the current overdose epidemic far longer than we’ve seen with previous epidemics.
“Availability of treatment is a crucial factor,” Ciccarone said, in allowing a decline in the overdose epidemic to take hold. Only about 1 in 3 people in drug treatment programs receive medication-assisted treatment, the most effective way to treat addiction disorders.
Some preliminary CDC data suggests that total drug overdoses have plateaued in the last year, driven by a decline in heroin and painkiller deaths; however, in the same time period, fentanyl deaths have continued to increase. A recent Blue Cross Blue Shield report found a 5% drop in clients reporting opioid use disorders as well.
Andrew Kolodny of Brandeis University told BuzzFeed News by email that the drop in new heroin users was “very good news,” not just for the sheer numbers, but also because it runs contrary to the theory that more people would turn to heroin as doctors became more cautious about prescribing opioid painkillers.
“The reason deaths have soared in illicit opioid users is because the illicit opioid supply became much more dangerous,” because of fentanyl, Kolodny said. “The new [survey] data makes this easier to see.”
While heroin use may be on a decline, there were some concerning upticks found in the survey. Methamphetamine use was found to be more popular among young adults 18 to 25 years old and pregnant women reported more opioid, cocaine, and marijuana use.
Despite it looking like things are heading in the right direction with the drop in new heroin users, the number of overdose fatalities remains “unacceptably high,” Ciccarone said.
Filed under: General Problems | 4 Comments »
SWEDESBORO, N.J.–(BUSINESS WIRE)–Sep 14, 2018–A nationwide survey shows that there are unintended consequences for veterinary medicine caused by the Drug Enforcement Administration’s (DEA) efforts to address the national opioid crisis. Opioids in animal medicine are the foundation, and often the only method, of pain control and anesthesia. They are critical for the treatment of animals that have been hit by a car, shot by a gun, mauled by another animal, undergone surgery, or suffer from a severe disease or other trauma. Most pet owners, regulators, elected officials, and state board of pharmacy members are not aware of the repercussions.
To address the mis-use and diversion of opioids by people, the DEA has proposed an average 10 percent decrease in the 2019 manufacturing quotas for six frequently abused opioids, including five key Class II opioid drugs commonly used by veterinarians. DEA decreased allowable opioid manufacturing quotas by 25 percent in 2017 and 20 percent this year. When supplies of these drugs are limited, manufacturers and distributors give preference to allocating their limited supplies for use in human health, creating shortages for veterinary medical practitioners. For example, in August, Pfizer suspended delivery of injectable opioids to veterinary customers.
According to the survey, these shortages have had the unintended results of creating unnecessary pain, suffering, and death of animals because alternatives are less effective and are more expensive.
Key findings of the survey:
In the past year, from 27% to 73% of veterinary professionals have had difficulty obtaining necessary supplies of five opioids they consider “important to your practice and to your patients’ health” by 50% – 80% of respondents. They include Hydromorphone, Morphine, Fentanyl, Hydrocodone, and Oxymorphone.Shortages of these opioids have caused … The use of less effective, non-narcotic alternatives such as NSAIDS (83%);Increased patient suffering (71%);Use of a local anesthetic (49%);Postponed procedures (26%); andPatient deaths (3%)88% of respondents “rarely” or “never” see the four warning signs published by DEA that a client is potentially abusing opioids. Nevertheless, 63% “have training and/or procedures in place for medical and other staff members to recognize the signs of opioid abuse.”
The survey was conducted in September by Wedgewood Pharmacy, the largest animal-health compounding pharmacy in the U.S. The invitation to participate went to 53,968 veterinary professionals; 1,135 completed the survey. The results (which include hundreds of write-in comments from veterinarians) will be included in formal comments that the company will submit to the DEA regarding the proposed production quota reductions. [DEA will be accepting comments at http://www.regulations.gov until 11:59PM, September 19, 2018. Please reference ‘‘Docket No. DEA–488P’’ on all correspondence, including any attachments.]
Michael Blaire, R.Ph., FIACP, vice president, Government and Regulatory Affairs noted, “Shortages limit therapeutic choices and are especially problematic given the number of species veterinarians treat—from tiny kittens to large dogs, horses, and even elephants—and how different species react to opioids or their alternatives. Shortages demand that veterinarians frequently change medications and pain-management protocols, and this increases the risk of medical errors. While we applaud DEA’s efforts to address the national opioid crisis among humans, we’re asking them to be thoughtful about the impact the actions they take will have on the animal patients owned by 68% of American homes and the millions of animals in zoos, aquaria, stables, shelters, hospitals, research facilities, police and military facilities. We need to work together to address a national crisis in human health while continuing to provide veterinarians with the medicines they need to practice.”
One veterinarian wrote this comment to illustrate how opioid shortages affect his or her patients: “We have an emergency practice, so we see a lot of very painful animals from surgeries, traumas, and severe illness. Most of our patients in acute pain are not candidates for NSAIDS or other treatments like laser and acupuncture, which take longer to work and are not proven effective for severe pain. Not having access to opioids almost makes treatment cruel.”
Wedgewood Pharmacy and recently acquired Diamondback Drugs are licensed by DEA to manufacture controlled substances, which they do exclusively for animal patients. Compounded medications are created and prepared by specially trained pharmacists and pharmacy technicians in nationally accredited, state-regulated facilities, when mass-manufactured drugs are not available or appropriate for a patient. These medications are prescribed and dispensed under orders written by veterinarians. At least one facility has experienced difficulty obtaining the quantities of active pharmaceutical ingredients needed to meet the demands of their veterinary customers, because of purchasing quotas set by DEA.
The sampling of participants in the survey was participant-driven, not random, and therefore measures of statistical significance such as confidence levels and sampling error do not apply to the results of the study. They represent the opinions of the professionals who participated.
About Wedgewood Pharmacy
In its 37 years, Wedgewood Pharmacy has grown from a local community pharmacy to become one of the largest compounding pharmacies in the United States; it is the leading pharmacy in animal health. Wedgewood Pharmacy serves more than 50,000 prescribers and hundreds of thousands of patients throughout the U.S. every year.
George (late) and Lucy Malmberg, both pharmacists, purchased Wedgewood Pharmacy in 1981; the pharmacy was founded in 1980. In June 2016, Chicago-based New Harbor Capital became the majority owner of the company. In July 2018, the company acquired Diamondback Drugs, Scottsdale, Arizona.
Wedgewood Pharmacy is accredited by the Pharmacy Compounding Accreditation Board (PCAB ® ) for compliance with PCAB and other nationally recognized compounding standards. PCAB was formed by eight of the nation’s leading pharmacy associations and is a service of Accreditation Commission for Health Care. As a third-party accreditation organization, PCAB has developed the highest national standards against which providers are measured to demonstrate their ability to effectively and efficiently deliver quality compounded medications to consumers. Wedgewood Pharmacy employs more than 500 people in its state-of-the-art compounding pharmacies in Swedesboro, New Jersey and Scottsdale, Arizona.
View source version on businesswire.com:https://www.businesswire.com/news/home/20180914005480/en/
CONTACT: Wedgewood Pharmacy
Michael Blaire, R.Ph., FIACP
Vice President, Government and Regulatory Affairs
Filed under: General Problems | 7 Comments »