A Nevada doctor plans to sue Walmart after the big-box company told its patients it will no longer fill their prescriptions.
Dr. Gary Ridenour has been a Fallon doctor for more than 30 years. He’s a country doctor who still makes house calls.
“I like the smallness of the town. I like the people of the town. The simplicity of the town,” Ridenour said.
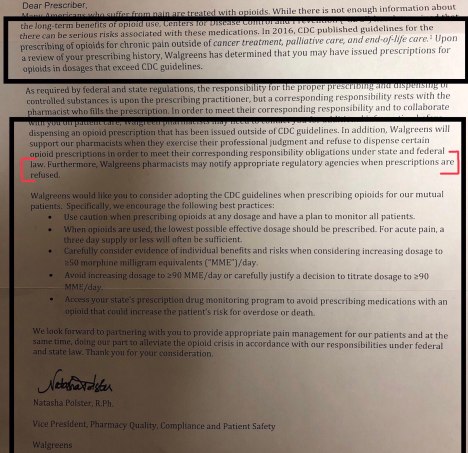
One day last summer he said the billion dollar company stomped on his small-town practice. Walmart sent Dr. Ridenour a letter that said, “In our efforts to meet our compliance obligations… and to help combat prescription drug abuse and diversion, we routinely review the prescribing patterns and practices of the prescribers whose prescriptions are presented to us for filling… we will not be able to continue filling your controlled substance prescriptions.”

Dr. Ridenour was surprised and upset.
“They said you can’t write prescriptions, controlled substances for any Walmart in the United States. Oh, that’s nice,” he said. “I got no phone call. I got no letter from these people, what are they doing? “
Walmart will no longer fill his controlled substances prescriptions like Fentanyl, Oxycodone and Hydrocodone. But it also won’t fill scripts for Valium, Xanax and cough medicine with Codeine.
Dr. Ridenour’s patients said they didn’t get any notice that Walmart wouldn’t fill their pain meds anymore.
“I couldn’t believe it,” Susan Harrison, a Fernley resident said.
Harrison said she was on a deck when it collapsed and crushed her leg and ankle. She said a surgeon had to put 12 pieces of steal in her body. Harrison said her orthopedic specialist asked Dr. Ridenour, her primary care physician, to continue her pain medication. Harris said she takes a half a pill in the morning and a half in the evening.
“If I didn’t have any pain pills I wouldn’t be able to get out of my bed in the morning. I wouldn’t be able to walk anywhere,” she said.
For nearly two months, News 4 has e-mailed, called and left messages with Walmart several times for an explanation as to why it won’t fill Dr. Ridenour’s prescriptions. The company has not commented. But a news release on Walmart’s website announced a new company policy that would restrict initial acute opioid prescriptions to no more than a seven-day supply. Dr. Gary Ridenour does prescribe beyond a seven-day supply.
Walmart is a private company and is not required to fill all prescriptions. But Dr. Ridenour’s patients say this is unfair.
“For Walmart to not understand what medical conditions people are coming in for and for just making assumptions without calling the physician and finding out that these people have real issues,” Harrison said.
Walmart is following the crack-down on opioids across the country. Nevada passed AB 474 that went into effect this year. The law requires prescribers do a risk assessment of the patient, run them through a state-wide database and justify the quantity written.
The Board of Pharmacy and The Nevada State Board of Medical Examiners are primarily responsible for enforcing the new law. Dr. Ridenour says neither state agency has ever investigated him for wrong doing. He says he’s planning on filing a lawsuit against Walmart.
“I’ve never overprescribed. In fact, this year we kicked out 12 patients because we drugged screened them and they had,” he said.
Doctors complain the new law makes more work for them. And in Dr. Ridenour’s case, he believes the law scared Walmart into no longer filling his patients’ prescriptions.
“It’s not fair to my patients,” he said.
It also limits where his patients can fill prescriptions.
“Most of us in small towns don’t have a lot of options,” Harrison said.
http://www.ncpanet.org/home/find-your-local-pharmacy

Like this:
Like Loading...
Filed under: General Problems | 11 Comments »


















 This is the CDC info. please email them your story or call them.
This is the CDC info. please email them your story or call them. Meningitis trial: Massachusetts board let NECC off with warnings
Meningitis trial: Massachusetts board let NECC off with warnings