

















 The “opioid crisis” is like a COIN.. there are two sides. All too many bureaucrats only want to address those who are addicted to using/abusing certain substances. Rx opiates peaked in 2011-2012 and they have already dropped by abt 60% by today, but opioid OD/poisoning has increased from abt 14,000 to over 100,000/yr, and the vast majority of those deaths’ toxicology showed 80%+ illegal fentanyl. One doesn’t need a supercomputer to figure out that when Rx opioids drop by >50% and opioid OD/poisoning is up abt SEVEN FOLD, there is little to no relationship between Rx opioids and addiction. Recently the DEA stated that <1% of pharma opioids are diverted. Yet, there is an on-going push to reduce the availability of Rx opioids to treat acute and chronic pain. How many other high acuity pts dealing with chronic health issues… do we as a country increasingly try to limit or deny appropriate therapy? – that is the other side of the opioid crisis “coin”
The “opioid crisis” is like a COIN.. there are two sides. All too many bureaucrats only want to address those who are addicted to using/abusing certain substances. Rx opiates peaked in 2011-2012 and they have already dropped by abt 60% by today, but opioid OD/poisoning has increased from abt 14,000 to over 100,000/yr, and the vast majority of those deaths’ toxicology showed 80%+ illegal fentanyl. One doesn’t need a supercomputer to figure out that when Rx opioids drop by >50% and opioid OD/poisoning is up abt SEVEN FOLD, there is little to no relationship between Rx opioids and addiction. Recently the DEA stated that <1% of pharma opioids are diverted. Yet, there is an on-going push to reduce the availability of Rx opioids to treat acute and chronic pain. How many other high acuity pts dealing with chronic health issues… do we as a country increasingly try to limit or deny appropriate therapy? – that is the other side of the opioid crisis “coin”
The claim that <1% of pharma opiates are diverted, does not address nor confirm that there are a untold number of chronic pain pts are being forced to live without proper pain management and often exist in a torturous level of pain, being forced/restricted to their house, chair or bed. Just like some criminals who are put on “home arrest”, but these chronic pain pts have committed NO CRIMES.
Earlier this year, 50 states’ Attorney General and others sued the top three drug wholesalers that control abt 80% of the pharmacy market and the top three chain pharmacies (CVS, Walmart, Walgreen). Neither lawsuit went to court/trial but all agreed to pay billions in fines – while admitting no wrong doing – but also agreed to reduce the control meds that are sold to pharmacies and or pharmacies will dispense.
Since most people needing to be prescribed controlled meds are disabled and/or would be disabled without their meds. My non-attorney opinion is that these very large corporations have signed an agreement to discriminate against a large number of people who are a covered entities under the Americans with Disability Act.
I have talked to other chronic pain advocates and all of us or having an increased number of chronic pain pts reaching out because of they are all of a sudden being denied their pain meds.
I recently heard of a state medical licensing board that one particular board member was PUSHING for “rapid weaning” – perhaps a euphemism for cold turkey withdrawal, and reportedly those pts who their prescribers were forced into doing this with their pts and reportedly their had been some deaths – particularly those pts who were concurrently taking a opioid, benzo, and muscle relaxant.
Some pharmacists seem to be imposing their “beliefs” into their “clinical decisions” .. here is one from today https://www.cnn.com/2022/08/02/us/minnesota-morning-after-pill-lawsuit/index.html
I had to get involved with two different pts and where the pharmacist would not look into the pt’s circumstances to adjudicate those circumstances to take care of the pt’s need. One pt ended up moving all her Rxs from a Rite Aid to a local independent and the other one the prescriber was on board, the PBM was on board and it would appear that the Pharmacist did not understand what was said or was just lying and claiming that the claim was being DENIED by the PBM. I got the pt to get in a conference call with the PBM representative, the pt and the pharmacist… and all of a sudden the Rx claim was “miraculously” approved and the pt got their necessary medications.
The increased number of pts now reaching out to various advocates for some sort of help/assistance, will probably convert into a similar increase in deaths from comorbidity complications – labeled as “natural causes” – from under/untreated pain and or suicides.
I would suggest that anyone who is reducing your meds, I would ask for the clinical rational IN WRITING why it is being done. If they reference the MME system as rational. Here is a article that pretty well explains that the MME system has no double blind clinical studies to support its conclusion https://www.acsh.org/news/2022/03/01/true-story-morphine-milligram-equivalents-mme-16154
I would ask them, what level/intensity of pain they expect you to live/exist in ? IMO, anything > 5, that is a torturous level of pain.
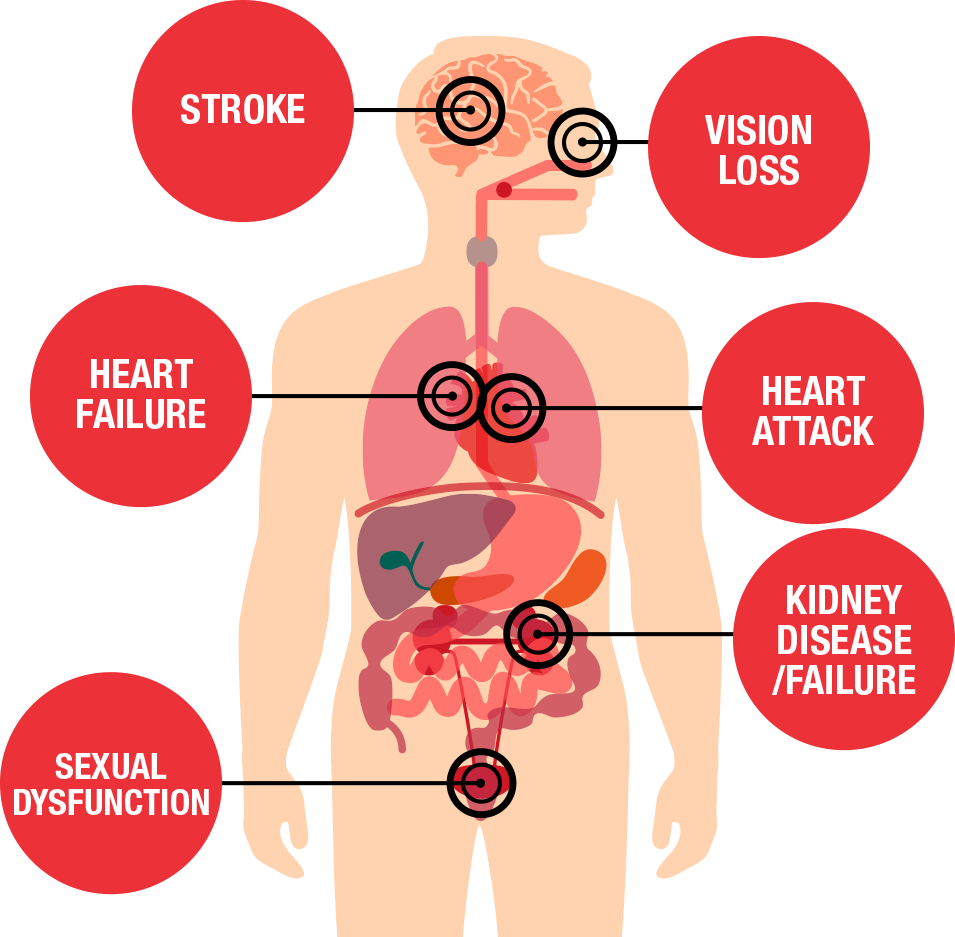
If, after your meds have been reduced and your blood pressure goes up and you end up on taking up to 4-5 different categories of pharma blood pressure medications and your elevated BP has little/no change… here is a graphic that shows what physical damage you can anticipate https://www.pharmaciststeve.com/wp-content/uploads/2022/01/htnsideeffects.png
Whatever practitioner you are dealing with, and they have a patient portal… do not be afraid to use it… use it to NUDGE them to give you a answer in writing, Share documentation, studies that suggests that you needed to be treated differently and you could improve your QOL, after all practitioner are suppose to be HEALERS.
I know that many of you have reached out to law firms. The times are changing dramatically towards those pts who have a valid medical necessity for being prescribed controlled meds. There are records of 3 major drug wholesalers and 3 large pharmacy chains ( CVS, Walmart, Walgreen) that signed agreements with 50 states’ attorney generals and others … that agreed in WRITING … to reduce the number of controls that the wholesalers sell to all pharmacies and those chains agreed to reduce the number of controlled meds they fill/dispense.
At face value, those agreements suggested that the reduction of control meds would be done indiscriminately with a broad brush.
If you don’t have access to a practitoner via a pt portal and if they won’t give you a answer in person. Send them a certified letter asking the question. If they refuse/decline to answer you in writing… One can presume that they really don’t have any real clinical rational to why they changed your therapy.
Share some of this information with your local media, reach out to law firms that deal with civil rights issues, because most likely you are not the only one being treated in the same manner from the same practitioner or all practitioners that are employed by the same large healthcare corporation, because they are obeying some corporate edict.
Filed under: General Problems | Leave a Comment »









{kind=link}